You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- MethDocument12 pagesMethJeremy WilliamsNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Cardiovascular DiseasesDocument8 pagesCardiovascular DiseasesRebecca MarshallNo ratings yet
- The End of Dieting by Joel Fuhrman, MD (Excerpt)Document22 pagesThe End of Dieting by Joel Fuhrman, MD (Excerpt)HarperOne (an imprint of HarperCollins)69% (13)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Savage Worlds - Ancient World - Bestiarum VocabulumDocument139 pagesSavage Worlds - Ancient World - Bestiarum VocabulumVictor Figueiredo100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Microbiology TablesDocument19 pagesMicrobiology TablesRebecca MarshallNo ratings yet
- Holistic Health QuestionnaireDocument28 pagesHolistic Health QuestionnaireMichael Grant WhiteNo ratings yet
- FUN1 Pharmacology TableDocument10 pagesFUN1 Pharmacology TableRebecca MarshallNo ratings yet
- RCSI Handbook of Clinical Medicine - V1, 2nd EdDocument574 pagesRCSI Handbook of Clinical Medicine - V1, 2nd EdRebecca Marshall86% (7)
- Manual Trigger Point Therapy and Dry Needling Top 30 MusclesDocument84 pagesManual Trigger Point Therapy and Dry Needling Top 30 MusclesManuela CormioNo ratings yet
- BambooDocument24 pagesBamboojcoppala4476100% (1)
- Govt. College of Nursing, Jodhpur: Lesson Plan TopicDocument14 pagesGovt. College of Nursing, Jodhpur: Lesson Plan Topicvikas takNo ratings yet
- Boards and Beyond TableDocument11 pagesBoards and Beyond TableRebecca MarshallNo ratings yet
- Perbandingan Metode Pada Pemeriksaan Penggolongan Darah Abo Dan RhesusDocument2 pagesPerbandingan Metode Pada Pemeriksaan Penggolongan Darah Abo Dan RhesusafniridwanNo ratings yet
- RCSI Clinical Examinations in Medicine 2018-19Document189 pagesRCSI Clinical Examinations in Medicine 2018-19Rebecca MarshallNo ratings yet
- RCSI Handbook of Clinical Medicine - V2, 2nd EdDocument566 pagesRCSI Handbook of Clinical Medicine - V2, 2nd EdRebecca Marshall100% (4)
- National Vector Borne Disease Control Programme (NVBDCP) : Presented By, Javed Khan Roll No:32Document21 pagesNational Vector Borne Disease Control Programme (NVBDCP) : Presented By, Javed Khan Roll No:32fathima AlfasNo ratings yet
- CVR PharmacologyDocument6 pagesCVR PharmacologyRebecca MarshallNo ratings yet
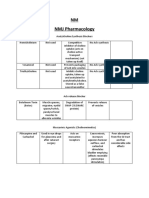
- NMJ PharmacologyDocument3 pagesNMJ PharmacologyRebecca MarshallNo ratings yet
- Drugs Mechanism Side Effect DiureticDocument3 pagesDrugs Mechanism Side Effect DiureticRebecca MarshallNo ratings yet
- Usmle Step 1 BreakdownDocument10 pagesUsmle Step 1 BreakdownRebecca MarshallNo ratings yet
- Thoughts After Amboss QbankDocument2 pagesThoughts After Amboss QbankRebecca MarshallNo ratings yet
- Neurotoxicity of E-CigarettesDocument15 pagesNeurotoxicity of E-CigarettesRebecca MarshallNo ratings yet
- From Women Food and HormonesDocument6 pagesFrom Women Food and HormonesDiana PintoNo ratings yet
- StreptokinaseDocument2 pagesStreptokinasePramod RawoolNo ratings yet
- Student Assessment 1Document10 pagesStudent Assessment 1mahaNo ratings yet
- Cervical Cancer StagingDocument3 pagesCervical Cancer StagingMeka Medina RahmanNo ratings yet
- Acmella OleraceaDocument3 pagesAcmella Oleraceajcoppala4476No ratings yet
- Northern Mindanao Medical Center Department of Obstetrics and Gynecology Schedule For November 2019Document8 pagesNorthern Mindanao Medical Center Department of Obstetrics and Gynecology Schedule For November 2019Janellah BatuaanNo ratings yet
- Chapter 3 Heredity and VariationDocument14 pagesChapter 3 Heredity and Variationuncleya07100% (1)
- Development of Safe Juices For Immunocompromised Patients by Irradiation Alone or in Combination With Other TechnologiesDocument245 pagesDevelopment of Safe Juices For Immunocompromised Patients by Irradiation Alone or in Combination With Other Technologies4negeroNo ratings yet
- Listening 6 Suzzane HindsDocument9 pagesListening 6 Suzzane HindsjamesNo ratings yet
- Lumbar Spinal Stenosis - Pathophysiology, Clinical Features, and DiagnosisDocument20 pagesLumbar Spinal Stenosis - Pathophysiology, Clinical Features, and DiagnosisVy Phạm Thị TrúcNo ratings yet
- Cell Biology Cell Structures and Their FunctionsDocument30 pagesCell Biology Cell Structures and Their FunctionsMing Shahir SalehNo ratings yet
- What Is BPA (Bisphenol A) - Is BPA Harmful - Medical News TodayDocument4 pagesWhat Is BPA (Bisphenol A) - Is BPA Harmful - Medical News Todayscribidvel1No ratings yet
- 2020 03 20 - Daily Safety Moment - Coronavirus (COVID-19) Update - No. 719BDocument2 pages2020 03 20 - Daily Safety Moment - Coronavirus (COVID-19) Update - No. 719BE. Ricardo Ponce EspejoNo ratings yet
- Hedge Papers 77 Pharmas Failed Promise Enviro Degradation CPD October 2022 FINALDocument44 pagesHedge Papers 77 Pharmas Failed Promise Enviro Degradation CPD October 2022 FINALMarcos Pérez-RamírezNo ratings yet
- Skizofrenia SimplexDocument8 pagesSkizofrenia SimplexUswatun KhasanahNo ratings yet
- GOD'S POWER IN THE NEW ANOINTING WATER AND STICKER - The Synagogue, Church of All Nations - SCOAN - Prophet T.B. Joshua (GeneralDocument1 pageGOD'S POWER IN THE NEW ANOINTING WATER AND STICKER - The Synagogue, Church of All Nations - SCOAN - Prophet T.B. Joshua (GeneralAnnette EastineNo ratings yet
- ES - Water PollutionDocument29 pagesES - Water PollutionVedant SharmaNo ratings yet
- Digeorge Syndrome: Rupesh Mohandas GR3Document18 pagesDigeorge Syndrome: Rupesh Mohandas GR3Rupesh MohandasNo ratings yet
- 11 Engcore22 23 sp01Document19 pages11 Engcore22 23 sp01vikram reddyNo ratings yet
- R V HennessyDocument7 pagesR V HennessyRachel Hii100% (1)
- 1,000,000 AND COUNTING: A July Without Roger FedererDocument16 pages1,000,000 AND COUNTING: A July Without Roger FedererrtNo ratings yet