You might also like
- PaCO2 UCIDocument8 pagesPaCO2 UCIDiana CarolinaNo ratings yet
- Oxigen Oter ApiaDocument16 pagesOxigen Oter ApiaDiana CarolinaNo ratings yet
- Veterinary Clinics: Hypoxemia: A Quick ReferenceDocument4 pagesVeterinary Clinics: Hypoxemia: A Quick ReferenceDiana CarolinaNo ratings yet
- Distress RespiratoriopdfDocument11 pagesDistress RespiratoriopdfDiana CarolinaNo ratings yet
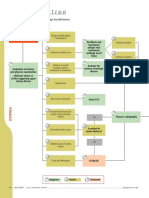
- Diagnostic Tree: DyspneaDocument2 pagesDiagnostic Tree: DyspneaDiana CarolinaNo ratings yet
- Veterinary Clinics: Hypoxemia: A Quick ReferenceDocument4 pagesVeterinary Clinics: Hypoxemia: A Quick ReferenceDiana CarolinaNo ratings yet
- Veterinary Clinics: Hypoxemia: A Quick ReferenceDocument4 pagesVeterinary Clinics: Hypoxemia: A Quick ReferenceDiana CarolinaNo ratings yet
- Analisis de Gases SanguineosDocument18 pagesAnalisis de Gases SanguineosDiana CarolinaNo ratings yet
- Veterinary Clinics: Hypoxemia: A Quick ReferenceDocument4 pagesVeterinary Clinics: Hypoxemia: A Quick ReferenceDiana CarolinaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Bob Jones: This CV Template Will Suit Jobseekers With Senior Management ExperienceDocument3 pagesBob Jones: This CV Template Will Suit Jobseekers With Senior Management ExperienceDickson AllelaNo ratings yet
- Perceptual Objective Listening Quality Assessment (POLQA), The Third Generation ITU-T Standard For End-to-End Speech Quality Measurement Part I-Temporal AlignmentDocument19 pagesPerceptual Objective Listening Quality Assessment (POLQA), The Third Generation ITU-T Standard For End-to-End Speech Quality Measurement Part I-Temporal AlignmentmewarulesNo ratings yet
- WB-Mech 120 Ch05 ModalDocument16 pagesWB-Mech 120 Ch05 ModalhebiyongNo ratings yet
- MHD Exam 6 MaterialDocument179 pagesMHD Exam 6 Materialnaexuis5467100% (1)
- Practical Econometrics Data Collection Analysis and Application 1st Edition Hilmer Test BankDocument27 pagesPractical Econometrics Data Collection Analysis and Application 1st Edition Hilmer Test Bankdavidhallwopkseimgc100% (28)
- 热虹吸管相变传热行为CFD模拟 王啸远Document7 pages热虹吸管相变传热行为CFD模拟 王啸远小黄包No ratings yet
- Adobe Scan 23-Feb-2024Document4 pagesAdobe Scan 23-Feb-2024muzwalimub4104No ratings yet
- Siemens 6SL31622AA000AA0 CatalogDocument20 pagesSiemens 6SL31622AA000AA0 CatalogIrfan NurdiansyahNo ratings yet
- Media Analysis-GraphicDocument1 pageMedia Analysis-Graphicapi-262266786100% (1)
- Motorola Phone Tools Test InfoDocument98 pagesMotorola Phone Tools Test InfoDouglaswestphalNo ratings yet
- Debug and AssemblerDocument9 pagesDebug and AssemblerManoj GurralaNo ratings yet
- Colombo Port City Causing Unimaginable Environmental HarmDocument6 pagesColombo Port City Causing Unimaginable Environmental HarmThavam RatnaNo ratings yet
- Physics Cheat SheetDocument8 pagesPhysics Cheat SheetJeremiah MoussaNo ratings yet
- Have Been Tried From Time To Time," As Churchill Famously Said (Third Paragraph) "?Document25 pagesHave Been Tried From Time To Time," As Churchill Famously Said (Third Paragraph) "?Aditya ThakurNo ratings yet
- Common Rail Injector Tester CR-C +S60H Multifunction Test MachineDocument3 pagesCommon Rail Injector Tester CR-C +S60H Multifunction Test MachineAlen HuangNo ratings yet
- Apache Nifi Tutorial - What Is - Architecture - InstallationDocument5 pagesApache Nifi Tutorial - What Is - Architecture - InstallationMario SoaresNo ratings yet
- Declaration of Absence of Conflict of InterestDocument1 pageDeclaration of Absence of Conflict of InterestJvhelcoronacondat CondatNo ratings yet
- ĐÁP ÁN ĐỀ THI THỬ SỐ 03 (2019-2020)Document8 pagesĐÁP ÁN ĐỀ THI THỬ SỐ 03 (2019-2020)Đào VânNo ratings yet
- UST Corporation Law Syllabus 2020 2021Document26 pagesUST Corporation Law Syllabus 2020 2021PAMELA ALEXIA CASTILLONo ratings yet
- Culture Performance and Economic Return of Brown ShrimpDocument8 pagesCulture Performance and Economic Return of Brown ShrimpLuã OliveiraNo ratings yet
- Pursanova IXC ManualDocument16 pagesPursanova IXC ManualHector Serrano MagañaNo ratings yet
- Concordance C Index - 2 PDFDocument8 pagesConcordance C Index - 2 PDFnuriyesanNo ratings yet
- FORM 2 Enrolment Form CTU SF 2 v.4 1Document1 pageFORM 2 Enrolment Form CTU SF 2 v.4 1Ivy Mie HerdaNo ratings yet
- Certification Programs: Service As An ExpertiseDocument5 pagesCertification Programs: Service As An ExpertiseMaria RobNo ratings yet
- Implementasi Sistem Pengenalan Candi Kecil Di Yogyakarta Menggunakan BerbasisDocument7 pagesImplementasi Sistem Pengenalan Candi Kecil Di Yogyakarta Menggunakan BerbasisRivan AuliaNo ratings yet
- Worship Aid - May Crowning 2020Document5 pagesWorship Aid - May Crowning 2020Kevin RyanNo ratings yet
- Rights of An Accused Under Custodial InvestigationDocument17 pagesRights of An Accused Under Custodial Investigationadrianfrancis9100% (1)
- Report Palazzetto Croci SpreadsDocument73 pagesReport Palazzetto Croci SpreadsUntaru EduardNo ratings yet
- Free DMAIC Checklist Template Excel DownloadDocument5 pagesFree DMAIC Checklist Template Excel DownloadErik Leonel LucianoNo ratings yet
- Steve Talbott Getting Over The Code DelusionDocument57 pagesSteve Talbott Getting Over The Code DelusionAlexandra DaleNo ratings yet