You might also like
- Speech-Language Pathologist Involvement in Multi-Tiered System of Supports Questionnaire: Advances in Interprofessional PracticeDocument27 pagesSpeech-Language Pathologist Involvement in Multi-Tiered System of Supports Questionnaire: Advances in Interprofessional PracticeValentina Jara CalderónNo ratings yet
- Cooperation Between Occupational Health Services and Small-Scale Enterprises in Norway and SwedenDocument17 pagesCooperation Between Occupational Health Services and Small-Scale Enterprises in Norway and SwedenValentina Jara CalderónNo ratings yet
- Median Pitch: 260.372 HZ Mean Pitch: 234.375 HZ Standard Deviation: 52.449 HZ Minimum Pitch: 75.665 HZDocument17 pagesMedian Pitch: 260.372 HZ Mean Pitch: 234.375 HZ Standard Deviation: 52.449 HZ Minimum Pitch: 75.665 HZValentina Jara CalderónNo ratings yet
- Salud Ocupacional Interdisciplinariedad Seguridad Y Salud en El TrabajoDocument9 pagesSalud Ocupacional Interdisciplinariedad Seguridad Y Salud en El TrabajoValentina Jara CalderónNo ratings yet
- Dysphagia - Management in Adults and Children (Speech Pathology)Document22 pagesDysphagia - Management in Adults and Children (Speech Pathology)Valentina Jara Calderón100% (1)
- Asymmetrical Hearing Loss and Mega Cisterna Magna: A Case StudyDocument5 pagesAsymmetrical Hearing Loss and Mega Cisterna Magna: A Case StudyValentina Jara CalderónNo ratings yet
- Content ServerDocument30 pagesContent ServerValentina Jara CalderónNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
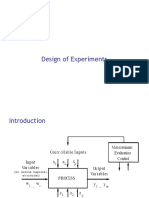
- Design of ExperimentDocument49 pagesDesign of ExperimentMuhammad Insan KamilNo ratings yet
- Department of Business Admin-16Document10 pagesDepartment of Business Admin-16api-338413336No ratings yet
- Kanchan Chopra, C H Hanumantha Rao-Growth, Equity, Environment and Population - Economic and Sociological Perspectives (Studies in Economic and Social Development) (2008)Document486 pagesKanchan Chopra, C H Hanumantha Rao-Growth, Equity, Environment and Population - Economic and Sociological Perspectives (Studies in Economic and Social Development) (2008)dianita conejitaNo ratings yet
- CRA 2010-Poster-PresentationsDocument236 pagesCRA 2010-Poster-PresentationsJoe GassNo ratings yet
- The Six Types of Socratic QuestionsDocument2 pagesThe Six Types of Socratic QuestionsBuketNo ratings yet
- Value Chain Analaysis of Tomato in Jaldu Woreda Centeral Ambo Zone Oromia Region EthiopiaDocument16 pagesValue Chain Analaysis of Tomato in Jaldu Woreda Centeral Ambo Zone Oromia Region EthiopiaMehari TemesgenNo ratings yet
- Cigre TrafoDocument11 pagesCigre Trafoluis900000No ratings yet
- MCQ On Human Resource ManagementDocument12 pagesMCQ On Human Resource ManagementAman Kumar satapathy50% (14)
- Bpac-101: Perspectives On Public AdministrationDocument15 pagesBpac-101: Perspectives On Public AdministrationDiksha UniyalNo ratings yet
- 4 Three Way Factorial AnovaDocument21 pages4 Three Way Factorial AnovaJestoni Dulva ManiagoNo ratings yet
- Hanushek and WoesmanDocument65 pagesHanushek and Woesmanjoeflynn362No ratings yet
- Globalisasi Budaya Dan Tantangan Untuk Teori Komunikasi TradisionalDocument18 pagesGlobalisasi Budaya Dan Tantangan Untuk Teori Komunikasi Tradisionalrahmad08No ratings yet
- Political Cycle - Alberto AlesinaDocument3 pagesPolitical Cycle - Alberto AlesinayumicintaNo ratings yet
- Teacher Education: Quirino State UniversityDocument11 pagesTeacher Education: Quirino State UniversityNoralyn Ulnagan ParditoNo ratings yet
- The Influence of Corporate Social Responsibility On Incumbent Employees: A Meta-Analytic Investigation of The Mediating and Moderating MechanismsDocument33 pagesThe Influence of Corporate Social Responsibility On Incumbent Employees: A Meta-Analytic Investigation of The Mediating and Moderating MechanismsDuaa ZahraNo ratings yet
- Impactof ATMbankingperformanceoncustomersatisfactionwiththebankin MalawiDocument10 pagesImpactof ATMbankingperformanceoncustomersatisfactionwiththebankin MalawiThanga DuraiNo ratings yet
- Confidence Intervals: Example: Average HeightDocument7 pagesConfidence Intervals: Example: Average HeightJoanne Bernadette IcaroNo ratings yet
- Forest Park High School Data Inventory Mykea YoungDocument3 pagesForest Park High School Data Inventory Mykea Youngapi-608836622No ratings yet
- Chapter 8 - MergedDocument61 pagesChapter 8 - MergedKyo learnNo ratings yet
- A Y A: I I D A F S P ?: Gility in Oung Thletes S TA Ifferent Bility ROM Peed and OwerDocument9 pagesA Y A: I I D A F S P ?: Gility in Oung Thletes S TA Ifferent Bility ROM Peed and OwerVladimir PokrajčićNo ratings yet
- Welcome To Our Research Class!Document19 pagesWelcome To Our Research Class!IzumiNo ratings yet
- Business Analytics & Text Mining Modeling Using Python: Dr. Gaurav DixitDocument17 pagesBusiness Analytics & Text Mining Modeling Using Python: Dr. Gaurav DixitRamuNo ratings yet
- VP Business Development Eclinical Applications in Nashville TN Resume John HedbergDocument2 pagesVP Business Development Eclinical Applications in Nashville TN Resume John HedbergJohnHedbergNo ratings yet
- CV - Pelle SommanssonDocument1 pageCV - Pelle SommanssonpellesommanssonNo ratings yet
- Pathik Desai Resume PDFDocument1 pagePathik Desai Resume PDFpathik desaiNo ratings yet
- Report PDFDocument136 pagesReport PDFditapermatasariNo ratings yet
- Obstructive Sleep Apnea ThesisDocument8 pagesObstructive Sleep Apnea Thesisjeanniesuttonminneapolis100% (2)
- Ethics Reference GuideDocument25 pagesEthics Reference GuideAJay LevantinoNo ratings yet
- Ch14 Anthropometry and Bio Mechanics Oct2009Document62 pagesCh14 Anthropometry and Bio Mechanics Oct2009rwjerniganNo ratings yet
- PHILHIS Chapter 1 2Document23 pagesPHILHIS Chapter 1 2aldwin RamirezNo ratings yet