You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- MCBU - Lifting & Rigging Questions and AnswersDocument15 pagesMCBU - Lifting & Rigging Questions and AnswersBhaiJan59No ratings yet
- Progress Chart SMAW NC IIDocument11 pagesProgress Chart SMAW NC IIpauline nuegaNo ratings yet
- Pakarab Fertilizers IT Help Desk FormDocument1 pagePakarab Fertilizers IT Help Desk FormHamzaNoumanNo ratings yet
- Elevator Rescue PlanDocument7 pagesElevator Rescue Planzardoz314100% (1)
- One Direct Method Statement: Preventative MeasuresDocument4 pagesOne Direct Method Statement: Preventative MeasuresAyu Wanda SaraswatiNo ratings yet
- EP-HQ-GDL-008-00 Safety - Critical - Elements - Integrity - Management - GuidelineDocument57 pagesEP-HQ-GDL-008-00 Safety - Critical - Elements - Integrity - Management - GuidelineAHMED AMIRA100% (5)
- Scaffolding: Submitted By, Akhilesh.A Production Operator (TR), Forbes Bumiarmada LimitedDocument42 pagesScaffolding: Submitted By, Akhilesh.A Production Operator (TR), Forbes Bumiarmada LimitedHamzaNoumanNo ratings yet
- What Are Assignment Instruction and SOP?Document3 pagesWhat Are Assignment Instruction and SOP?kanwoNo ratings yet
- Fire and Life Safety Director FLSD CurriculumDocument481 pagesFire and Life Safety Director FLSD CurriculumAnna PierceNo ratings yet
- HIRADCDocument16 pagesHIRADCyono Daryono100% (2)
- What Is A Risk Assessment?Document7 pagesWhat Is A Risk Assessment?Mohamad Yusof0% (1)
- Fire Safety in High Rise Hotel BuildingsDocument2 pagesFire Safety in High Rise Hotel BuildingsArnoldNo ratings yet
- Jazetal Gloss-MsdsDocument5 pagesJazetal Gloss-MsdsMahmoud Flefil100% (1)
- The ABC of NDTDocument5 pagesThe ABC of NDTHamzaNoumanNo ratings yet
- Best Practices in Machinery InstallationDocument2 pagesBest Practices in Machinery InstallationHamzaNoumanNo ratings yet
- 2005 Nondestructive Testing Guide Equipment Condition AssessmentDocument8 pages2005 Nondestructive Testing Guide Equipment Condition AssessmentHamzaNoumanNo ratings yet
- Balance Plot FormDocument1 pageBalance Plot FormHamzaNoumanNo ratings yet
- Helium Leak Detector vs Pressure Decay Leak Testing MethodsDocument2 pagesHelium Leak Detector vs Pressure Decay Leak Testing MethodsHamzaNoumanNo ratings yet
- Shift 2 Schedule (Sept 12 - Sept 20 '22)Document1 pageShift 2 Schedule (Sept 12 - Sept 20 '22)HamzaNoumanNo ratings yet
- H Hole MesaurmentDocument2 pagesH Hole MesaurmentHamzaNoumanNo ratings yet
- Acceptance Criteria of Weld Defects As Per Different CodesDocument17 pagesAcceptance Criteria of Weld Defects As Per Different CodesShubham ShuklaNo ratings yet
- Bayyinat ArticleDocument4 pagesBayyinat ArticleHamzaNoumanNo ratings yet
- Congratulations On Your Completion: Hamza NomanDocument1 pageCongratulations On Your Completion: Hamza NomanHamzaNoumanNo ratings yet
- Fluid Handling System PriceDocument2 pagesFluid Handling System PriceHamzaNoumanNo ratings yet
- Nbo-Tc NewDocument24 pagesNbo-Tc NewHamzaNoumanNo ratings yet
- Certificate of Completion: Hafiz NomanDocument1 pageCertificate of Completion: Hafiz NomanHamzaNoumanNo ratings yet
- Confirmation - Check-InDocument1 pageConfirmation - Check-InHamzaNoumanNo ratings yet
- MC LiftRigBestPractices Poster 11X17Document1 pageMC LiftRigBestPractices Poster 11X17HamzaNoumanNo ratings yet
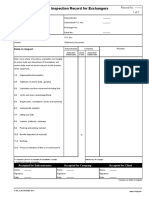
- 7 22 2022 Mech - 19596Document1 page7 22 2022 Mech - 19596HamzaNoumanNo ratings yet
- Onboarding Checklist: Best Practices for a Smooth StartDocument1 pageOnboarding Checklist: Best Practices for a Smooth StartHamzaNoumanNo ratings yet
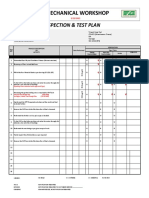
- Mechanical Workshop: Inspection & Test PlanDocument4 pagesMechanical Workshop: Inspection & Test PlanHamzaNoumanNo ratings yet
- Cylinder Test-Certification-ProceduresDocument3 pagesCylinder Test-Certification-ProceduresHamzaNoumanNo ratings yet
- Calculate your daily water intake based on weightDocument7 pagesCalculate your daily water intake based on weightSuyenthan SathishNo ratings yet
- Manpower Workshop Garage CraftDocument7 pagesManpower Workshop Garage CraftHamzaNoumanNo ratings yet
- Sr. No. Description Unit: Workshop / Garage Craft IssuesDocument14 pagesSr. No. Description Unit: Workshop / Garage Craft IssuesHamzaNoumanNo ratings yet
- Contract Extension of Hafiz Hussain 2021Document2 pagesContract Extension of Hafiz Hussain 2021HamzaNoumanNo ratings yet
- Advance Cash For Cricket PitchDocument1 pageAdvance Cash For Cricket PitchHamzaNoumanNo ratings yet
- JSA For Woma Jet TestingDocument2 pagesJSA For Woma Jet TestingHamzaNoumanNo ratings yet
- D Level Safety Meeting Quality Checklist - RevisedDocument1 pageD Level Safety Meeting Quality Checklist - RevisedHamzaNoumanNo ratings yet
- 6 Establish Verification ProceduresDocument6 pages6 Establish Verification ProceduresAndre MarsNo ratings yet
- Rqa 0009 TXDDocument22 pagesRqa 0009 TXDserga333No ratings yet
- Back To Basic: The Six Rules For Supervisor To Reinforce HseDocument8 pagesBack To Basic: The Six Rules For Supervisor To Reinforce Hseanjas bahridNo ratings yet
- MSDS PerliteDocument5 pagesMSDS Perlitenaidu60606No ratings yet
- CRC Smoke Test SDSDocument9 pagesCRC Smoke Test SDSA RNo ratings yet
- Aquaculture Checklist Edition 9Document109 pagesAquaculture Checklist Edition 9elflaquito80No ratings yet
- Job Safety Analysis (JSA) Risk AssessmentDocument3 pagesJob Safety Analysis (JSA) Risk AssessmentnbvillarazoNo ratings yet
- Chapter 1Document68 pagesChapter 1khurramNo ratings yet
- Material Safety Datasheet FOAMS WITH CHLORPARAFFINE EN Material Safety Datasheet IBD WWI 00000000000005001078 000Document12 pagesMaterial Safety Datasheet FOAMS WITH CHLORPARAFFINE EN Material Safety Datasheet IBD WWI 00000000000005001078 000AbidNo ratings yet
- Sample Car PolicyDocument6 pagesSample Car PolicyJohn StewartNo ratings yet
- Fds Industria Alimentaria enDocument13 pagesFds Industria Alimentaria enGustavo Toledo BruzualNo ratings yet
- Instruction Book Xa (T) S 67-97 DD c3 Xa (T) S 130-185 Dd7 c3 App 2954 2150 07 enDocument116 pagesInstruction Book Xa (T) S 67-97 DD c3 Xa (T) S 130-185 Dd7 c3 App 2954 2150 07 enChester Dalitso MwanzaNo ratings yet
- Material Safety Data Sheet AC - 770 Class B Base: MSDS No: 37702-09 Effective: 02/09/09 Supercedes: 12/12/07 Page: 1 of 5Document5 pagesMaterial Safety Data Sheet AC - 770 Class B Base: MSDS No: 37702-09 Effective: 02/09/09 Supercedes: 12/12/07 Page: 1 of 5NICKYNo ratings yet
- Risk Assessment For Stone WorkDocument17 pagesRisk Assessment For Stone WorkKhuda BukshNo ratings yet
- 0151 Hazmat Imdg Code AdvancedDocument2 pages0151 Hazmat Imdg Code Advancedigorkubelzis0% (1)
- TM500TRE.00-ENG - Introduction To Integrated Safety - V4330Document40 pagesTM500TRE.00-ENG - Introduction To Integrated Safety - V4330FrancescoNo ratings yet
- Sample Occupational Safety and Health Management Plan Free Download - 2Document15 pagesSample Occupational Safety and Health Management Plan Free Download - 2Ahmed MohammedNo ratings yet
- PSM 3.1 - Understanding Hazards (v4)Document47 pagesPSM 3.1 - Understanding Hazards (v4)Ahmed HamadNo ratings yet
- South Metro Fire Rescue Authority Accreditation ReportDocument50 pagesSouth Metro Fire Rescue Authority Accreditation ReportRonda ScholtingNo ratings yet
- BAMnuttall Guidance For Contractors BookletDocument16 pagesBAMnuttall Guidance For Contractors BookletRichard TaffsNo ratings yet