You might also like
- Technology in Practical Dermatology: Non-Invasive Imaging, Lasers and Ulcer ManagementFrom EverandTechnology in Practical Dermatology: Non-Invasive Imaging, Lasers and Ulcer ManagementMichele FimianiNo ratings yet
- Laser & Light Therapy GuideDocument27 pagesLaser & Light Therapy Guidemiranda salimNo ratings yet
- Hemangiomas, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHemangiomas, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Sclerotherapy Information and Consent FormDocument3 pagesSclerotherapy Information and Consent FormDaniel DePrince IIINo ratings yet
- Fractional Laser: Santi Devina Pembimbing: Dr. Lynda Hariani, Sp. Bp-Re Textbook Reading 12 Februari 2016Document27 pagesFractional Laser: Santi Devina Pembimbing: Dr. Lynda Hariani, Sp. Bp-Re Textbook Reading 12 Februari 2016Habibie AinunNo ratings yet
- Oral Propranolol Effective Treatment Infantile HemangiomaDocument18 pagesOral Propranolol Effective Treatment Infantile HemangiomaneonitesNo ratings yet
- Understanding Hemangiomas: Causes, Types and TreatmentsDocument18 pagesUnderstanding Hemangiomas: Causes, Types and Treatmentsplastic guardiansNo ratings yet
- Dr. Mario Rivera, Zdenko Vizintin - Laser GynecologyDocument13 pagesDr. Mario Rivera, Zdenko Vizintin - Laser GynecologyancaberescuNo ratings yet
- Treatment Periorbital HiperpigmentationDocument8 pagesTreatment Periorbital HiperpigmentationDuta Patria HutamaNo ratings yet
- Morphology and Differential Diagnosis Skin Lesions GuideDocument92 pagesMorphology and Differential Diagnosis Skin Lesions GuideSami OmerNo ratings yet
- CP 111Document246 pagesCP 111Yhr YhNo ratings yet
- Sec 4 - Techniques 2Document31 pagesSec 4 - Techniques 2Karem TubeNo ratings yet
- Chronic Wounds PowerpointDocument34 pagesChronic Wounds PowerpointAnin DitaNo ratings yet
- Lasers in SurgeryDocument22 pagesLasers in Surgerynuclearbrain11No ratings yet
- 2009 4 Laser Lipolysis 1 0Document13 pages2009 4 Laser Lipolysis 1 0aillNo ratings yet
- Lipolytic Laser: Price, Effectiveness and ContraindicationsDocument1 pageLipolytic Laser: Price, Effectiveness and ContraindicationsDaniel Fajardo VilacháNo ratings yet
- Gynecomastia Surgery - Power Assisted LiposuctionDocument4 pagesGynecomastia Surgery - Power Assisted LiposuctionAlfredo Callanta,M.D.No ratings yet
- LiposuctionDocument8 pagesLiposuctionnikitagustiNo ratings yet
- Management of Hyperpigmentation of Lips With 940 NM Diode Laser: Two Case ReportsDocument8 pagesManagement of Hyperpigmentation of Lips With 940 NM Diode Laser: Two Case ReportsMadhu HariharanNo ratings yet
- HIFU ConsentDocument1 pageHIFU ConsentthraldorNo ratings yet
- Causes and Effects of Acne on Teenagers' Self-Esteem and Social LivesDocument16 pagesCauses and Effects of Acne on Teenagers' Self-Esteem and Social LivesLemuel KimNo ratings yet
- Hemangiomas: A Guide To UnderstandingDocument12 pagesHemangiomas: A Guide To UnderstandingChristian Marcelo MartinezNo ratings yet
- Tumescent TAPP Laparoscopic Inguinal Hernia RepairDocument6 pagesTumescent TAPP Laparoscopic Inguinal Hernia RepairUmer KhanNo ratings yet
- Pigmentary Disorders in Asian Skin Treatment With Laser and Intense Pulsed Light SourcesDocument8 pagesPigmentary Disorders in Asian Skin Treatment With Laser and Intense Pulsed Light SourcesLutfi MKNo ratings yet
- A Practical Guide To Dermal Filler Procedures: January 2012Document2 pagesA Practical Guide To Dermal Filler Procedures: January 2012Velibor StankovićNo ratings yet
- UntitledDocument147 pagesUntitledRianna MariaNo ratings yet
- Rejuvenating Facial Treatment with PRPDocument14 pagesRejuvenating Facial Treatment with PRPHend Abdalla100% (1)
- See Full Prescribing Information For Complete Boxed WarningDocument22 pagesSee Full Prescribing Information For Complete Boxed WarningTracy PopeNo ratings yet
- Wound DressingDocument27 pagesWound DressingUteNo ratings yet
- Antioxidants and Growth Factors in The Treatment of Alopecia With InjectablesDocument4 pagesAntioxidants and Growth Factors in The Treatment of Alopecia With InjectablesMedtext PublicationsNo ratings yet
- Skin Diseases Affecting The VulvaDocument7 pagesSkin Diseases Affecting The VulvaNoraNo ratings yet
- Dermaroller FaqsDocument9 pagesDermaroller Faqsjp516No ratings yet
- Botulinum Toxin InjectionsDocument7 pagesBotulinum Toxin InjectionsWalid YounesNo ratings yet
- Phototherapy For Dermatologic ConditionsDocument18 pagesPhototherapy For Dermatologic ConditionsSeth MosebyNo ratings yet
- Mesotherapy Poster PDFDocument2 pagesMesotherapy Poster PDFgemm88No ratings yet
- Liposuction SurgeryDocument12 pagesLiposuction SurgerynainacurthberrtNo ratings yet
- A Randomised Controlled Study For The Treatment of Acne Vulgaris Using High Intensity 414nm Solid State Diode ArraysDocument29 pagesA Randomised Controlled Study For The Treatment of Acne Vulgaris Using High Intensity 414nm Solid State Diode ArraysCaerwyn AshNo ratings yet
- Electro-Optical Synergy (ELOS) Technology For Combined Acne Scars PDFDocument4 pagesElectro-Optical Synergy (ELOS) Technology For Combined Acne Scars PDFAryantii AntyNo ratings yet
- Plasma Skin Regeneration Technology PDFDocument3 pagesPlasma Skin Regeneration Technology PDFLuiz Camargo JuniorNo ratings yet
- Photofacials Candela Ellipse IPL Technology - White-PaperDocument5 pagesPhotofacials Candela Ellipse IPL Technology - White-PaperRogier van der HeideNo ratings yet
- Cellulite Current Treatments, New Technology, And.3Document7 pagesCellulite Current Treatments, New Technology, And.3BoeroNo ratings yet
- Update On The Management of Keloids: A. Paul Kelly, MDDocument6 pagesUpdate On The Management of Keloids: A. Paul Kelly, MDBudi KusumaNo ratings yet
- Serdev Suture Techniques Breast Lift - Prof Nikolay P Serdev MD PHDDocument4 pagesSerdev Suture Techniques Breast Lift - Prof Nikolay P Serdev MD PHDjobetobaNo ratings yet
- PRP Review TemplateDocument15 pagesPRP Review TemplatedermoNo ratings yet
- Scars How Do We Grade ThemDocument6 pagesScars How Do We Grade Themdiana romeroNo ratings yet
- Hyperpigmentation Guide- Types, Tips & TreatmentsDocument10 pagesHyperpigmentation Guide- Types, Tips & TreatmentsN SubhashNo ratings yet
- IKD6 - Contrast Associated AKIDocument44 pagesIKD6 - Contrast Associated AKIRenal Association MauritiusNo ratings yet
- Acute Purulent Diseases of Fingers and HandDocument23 pagesAcute Purulent Diseases of Fingers and Handluckyswiss7776848No ratings yet
- Fat Reduction. Pathophysiology and Treatment Strategies (Liposuction)Document13 pagesFat Reduction. Pathophysiology and Treatment Strategies (Liposuction)Anonymous LnWIBo1GNo ratings yet
- Plastic Surgery: Understanding Abdominoplasty and LiposuctionDocument14 pagesPlastic Surgery: Understanding Abdominoplasty and LiposuctiondoctorbanNo ratings yet
- Plastic SurgeryDocument6 pagesPlastic SurgeryYing Hui LiewNo ratings yet
- Jett Plasma Lift Medical Manual ENG - Akt - .9.9.15 PDFDocument27 pagesJett Plasma Lift Medical Manual ENG - Akt - .9.9.15 PDFMichaely Natali100% (1)
- Omalizumab for Chronic Spontaneous UrticariaDocument35 pagesOmalizumab for Chronic Spontaneous UrticariaDeval MistryNo ratings yet
- Cutaneous Leishmaniasis: A Case StudyDocument7 pagesCutaneous Leishmaniasis: A Case StudyIJAR JOURNALNo ratings yet
- Treatment of Acne Scarring Mixed ArticlesDocument10 pagesTreatment of Acne Scarring Mixed ArticlesEWANo ratings yet
- Chemical CarcinogenesisDocument28 pagesChemical CarcinogenesisChama TlauNo ratings yet
- Breast CancerDocument18 pagesBreast CancerJohn AlcantaraNo ratings yet
- Sclerotherapy German GuidelinesDocument8 pagesSclerotherapy German GuidelinesGabriela DrăgoiNo ratings yet
- Postvagotomy and Postgastrectomy SyndromesDocument66 pagesPostvagotomy and Postgastrectomy SyndromesCanan YilmazNo ratings yet
- CA EndometriumDocument46 pagesCA EndometriumNovianaHartikasariNo ratings yet
- 2020 - Treatment of Melasma A Review of Less Commonly Used AntioxidantsDocument8 pages2020 - Treatment of Melasma A Review of Less Commonly Used Antioxidantsnancyerlen100% (1)
- 2020 - Pemphigus Vulgaris and Bullous Pemphigoid Update On Diagnosis and TreatmentDocument12 pages2020 - Pemphigus Vulgaris and Bullous Pemphigoid Update On Diagnosis and TreatmentnancyerlenNo ratings yet
- Sesion 3 Articulo Seminario 2 PsoriasisDocument16 pagesSesion 3 Articulo Seminario 2 PsoriasisQuispe Canares MariangelesNo ratings yet
- 2020 - Topical Ketokonazol For Androgenetic Alopecia A Systematic ReviewDocument6 pages2020 - Topical Ketokonazol For Androgenetic Alopecia A Systematic ReviewnancyerlenNo ratings yet
- 10 1016@j Clindermatol 2019 01 007 PDFDocument10 pages10 1016@j Clindermatol 2019 01 007 PDFMira GNo ratings yet
- 2021 - Dermoscopic Approach To Hypopigmentary or Depigmentary Lesion of Skin ColorDocument5 pages2021 - Dermoscopic Approach To Hypopigmentary or Depigmentary Lesion of Skin ColornancyerlenNo ratings yet
- Cutaneous Manifestations of COVID 19 An Evidence Based ReviewDocument13 pagesCutaneous Manifestations of COVID 19 An Evidence Based ReviewfikarNo ratings yet
- 2021 - Neonatal Dermatology The Normal, The Common and The SeriousDocument14 pages2021 - Neonatal Dermatology The Normal, The Common and The SeriousnancyerlenNo ratings yet
- Cutaneous Manifestations of COVID 19 An Evidence Based ReviewDocument13 pagesCutaneous Manifestations of COVID 19 An Evidence Based ReviewfikarNo ratings yet
- Tim Manning: How Drinking Hot Water and Avoiding Tea or Coffee Can Improve Your HealthDocument10 pagesTim Manning: How Drinking Hot Water and Avoiding Tea or Coffee Can Improve Your HealthTim ManningNo ratings yet
- One Word Answer Questions Covering DermatologyDocument5 pagesOne Word Answer Questions Covering DermatologyFan Eli50% (2)
- Medical Entomology MyiasisDocument6 pagesMedical Entomology MyiasisReda KhalafallaNo ratings yet
- Cryosurgery and ElectrosurgeryDocument51 pagesCryosurgery and ElectrosurgeryVeerabhadra RadhakrishnaNo ratings yet
- Chapter 5 Integumentary SystemDocument43 pagesChapter 5 Integumentary SystemThea MallariNo ratings yet
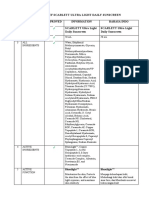
- PB - SCARLETT Ultra Light Daily SunscreenDocument4 pagesPB - SCARLETT Ultra Light Daily SunscreenArinda RamadhanaNo ratings yet
- The Red Palace by June HurDocument26 pagesThe Red Palace by June HurMacmillan Kids40% (5)
- Salsa Andhita Octavia - UASDocument21 pagesSalsa Andhita Octavia - UASsalsaNo ratings yet
- Forensic Classification of WoundsDocument5 pagesForensic Classification of WoundsSoze KeyserNo ratings yet
- Hydration of SkinDocument14 pagesHydration of SkinEhab AdelNo ratings yet
- OHR Spa Menu CITY Hotels Apr22Document9 pagesOHR Spa Menu CITY Hotels Apr22Shubham BNo ratings yet
- IFRA Certificate 49th - ALL LIMITS Palo SantoDocument4 pagesIFRA Certificate 49th - ALL LIMITS Palo SantoPhilippe BouchardNo ratings yet
- Brochure XGENIA ENGDocument2 pagesBrochure XGENIA ENGTaherNo ratings yet
- Proposal On Herbal Beauty Products by Simran PunjabiDocument2 pagesProposal On Herbal Beauty Products by Simran Punjabisimran punjabiNo ratings yet
- Tle (1) - Cosmetology ReviewerDocument15 pagesTle (1) - Cosmetology ReviewerNURASAN, CRYSTAL GAIL M.No ratings yet
- Word Sasbel 3Document6 pagesWord Sasbel 3Muhammad Naufal WidyatmakaNo ratings yet
- SLHT G9 BEAUTY CARE 3rd Quarter WEEK 3 4 PDFDocument6 pagesSLHT G9 BEAUTY CARE 3rd Quarter WEEK 3 4 PDFCarl Laura ClimacoNo ratings yet
- Dr. Advice Skin ItemsDocument20 pagesDr. Advice Skin ItemsRazia khatunNo ratings yet
- DERMAPENDocument33 pagesDERMAPENAriadna Roca100% (7)
- Premium Beauty and Personal Care in FranceDocument10 pagesPremium Beauty and Personal Care in FranceavaluehunterNo ratings yet
- Assessment of Sun-Related Behaviour, Knowledge and Attitudes Among Nursing StudentsDocument9 pagesAssessment of Sun-Related Behaviour, Knowledge and Attitudes Among Nursing StudentsAdrian Alexis Romero GuillenNo ratings yet
- Data of Doctors in TexasDocument54 pagesData of Doctors in TexasAdnanNo ratings yet
- Activity 2 Theoretical Practical CaseDocument4 pagesActivity 2 Theoretical Practical CaseScribdTranslationsNo ratings yet
- Rosacea GuideDocument24 pagesRosacea GuideMaría Celia Rocchetti100% (1)
- DLL q1 Week4 TleDocument7 pagesDLL q1 Week4 TleShane BisaNo ratings yet
- Secondary FormatDocument18 pagesSecondary FormatSayantan SahaNo ratings yet
- What Is FolliculitisDocument2 pagesWhat Is Folliculitisaashwini kumarNo ratings yet
- Tissue Engineering Advances for Skin Repair and RegenerationDocument14 pagesTissue Engineering Advances for Skin Repair and RegenerationRaniNo ratings yet
- Pityriasis Rubra Pilaris: A Clinical Review.: Dermatology Nursing / Dermatology Nurses' Association January 2006Document5 pagesPityriasis Rubra Pilaris: A Clinical Review.: Dermatology Nursing / Dermatology Nurses' Association January 2006Anonymous hxXpvZdZNo ratings yet
- Herbal.1Document27 pagesHerbal.1ahmunde2002No ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)