You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- 365 Journal Self DiscoveryDocument55 pages365 Journal Self DiscoveryAndromeda Sun100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Method of Testing Liquid Chillers: ANSI/ASHRAE Addendum A To ANSI/ASHRAE Standard 30-2019Document15 pagesMethod of Testing Liquid Chillers: ANSI/ASHRAE Addendum A To ANSI/ASHRAE Standard 30-2019Leandro Gabriel AndréNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Subaru Engines Eh65v ServiceDocument74 pagesSubaru Engines Eh65v ServicechrisrobinsoncnpNo ratings yet
- Lithium-Ion Battery Value Chain ReportDocument56 pagesLithium-Ion Battery Value Chain ReportSuhail100% (1)
- High Yield Biochemistry PDFDocument41 pagesHigh Yield Biochemistry PDFKyle Broflovski100% (2)
- Ebook PDF Theories of Personality 9th Edition by Jess Feist PDFDocument41 pagesEbook PDF Theories of Personality 9th Edition by Jess Feist PDFflossie.thompson26492% (37)
- Juwi Global PresentationDocument46 pagesJuwi Global PresentationMochamad BhadawiNo ratings yet
- Organic Mental Disorders Due To Brain DiseasesDocument45 pagesOrganic Mental Disorders Due To Brain DiseasesMEDS easyNo ratings yet
- Honors Chem Organic Chemistry NotesDocument3 pagesHonors Chem Organic Chemistry NotesWyatt KesterNo ratings yet
- FG52806 - 12-04-2010Document13 pagesFG52806 - 12-04-2010Roberto Carlos100% (1)
- Hp200rg SsDocument2 pagesHp200rg SsJad IssaNo ratings yet
- Building & Construction 2008Document8 pagesBuilding & Construction 2008firephoxNo ratings yet
- Electric Charges and Fields: Chapter OneDocument50 pagesElectric Charges and Fields: Chapter OnerockstarNo ratings yet
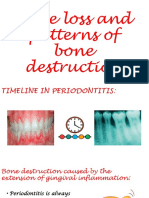
- Bone Loss and Patterns of Bone DestructionDocument21 pagesBone Loss and Patterns of Bone Destructionsonika selvarajNo ratings yet
- Internship Log Sheet Form 2023-W2Document1 pageInternship Log Sheet Form 2023-W2amglna2020No ratings yet
- Tra Ext FCN GR Gen 00017Document13 pagesTra Ext FCN GR Gen 00017Chandra MohanNo ratings yet
- Chapter 3: Partial Differentiation and Euler's Theorem: 3.1 Definitions of A Partial DerivativesDocument20 pagesChapter 3: Partial Differentiation and Euler's Theorem: 3.1 Definitions of A Partial DerivativesRimon SheikhNo ratings yet
- The Physical Fitness TestsDocument47 pagesThe Physical Fitness TestsBrittaney BatoNo ratings yet
- PMBLDC-Simulink - Permanent Magnet Brushless DC Motor Simulink Model.Document5 pagesPMBLDC-Simulink - Permanent Magnet Brushless DC Motor Simulink Model.Kidus DawitNo ratings yet
- Bhaktapur Case StudyDocument20 pagesBhaktapur Case StudyRaj K Pandey, MBS, MA, MPA75% (4)
- Fundamental Moral Theology - Fundamental OptionDocument2 pagesFundamental Moral Theology - Fundamental OptionJOHN REY MEMBELANo ratings yet
- MMW NotesDocument70 pagesMMW Notesp.dashaelaineNo ratings yet
- 1 s2.0 S0032386110010372 Main PDFDocument21 pages1 s2.0 S0032386110010372 Main PDFNia SyafiqqNo ratings yet
- F181 AC5 Proficiency Testing EQA Provider ISO IEC 17043 Application FormDocument4 pagesF181 AC5 Proficiency Testing EQA Provider ISO IEC 17043 Application FormJohnNo ratings yet
- Leopard Hills of India - Jawai SenaDocument2 pagesLeopard Hills of India - Jawai SenaKrisha ShahNo ratings yet
- Embedded RTOS Automotive Material 2020Document277 pagesEmbedded RTOS Automotive Material 2020Mohankumarglmanu MohankumarglmanuNo ratings yet
- A Ten Disk Procedure For The Detection of Antibiotic Resistance in EnterobacteriacaeDocument7 pagesA Ten Disk Procedure For The Detection of Antibiotic Resistance in EnterobacteriacaeNguyen Huu HienNo ratings yet
- Tensei Kenja No Isekai RaifuDocument594 pagesTensei Kenja No Isekai RaifugerrancioNo ratings yet
- Chapter 9 AnswersDocument3 pagesChapter 9 AnswersJose PopoffNo ratings yet
- Tute 3Document1 pageTute 3govind_misraaNo ratings yet