You might also like
- Zhu 2019Document9 pagesZhu 2019Blank Aguilar MNo ratings yet
- Clinical Applications of Nuclear Medicine Targeted TherapyFrom EverandClinical Applications of Nuclear Medicine Targeted TherapyEmilio BombardieriNo ratings yet
- Pharm Cvs ProdrugsDocument23 pagesPharm Cvs ProdrugsSindu SaiNo ratings yet
- CJCP08016 Rumboldt E372-E382Document12 pagesCJCP08016 Rumboldt E372-E382Diva DeviceNo ratings yet
- hr2008109 PDFDocument10 pageshr2008109 PDFKumarsai DurusojuNo ratings yet
- Blockers Remain First Choice in The Treatment Of: Should Primary Hypertension? A Meta-AnalysisDocument9 pagesBlockers Remain First Choice in The Treatment Of: Should Primary Hypertension? A Meta-AnalysisRahmat ullahNo ratings yet
- Nebivolol in HtaDocument16 pagesNebivolol in HtaCodruta Emanuela Maria VirsescuNo ratings yet
- s12245-021-00399-wDocument6 pagess12245-021-00399-wAlfonso Ga MaNo ratings yet
- Levosimendan in The Light of The Results of Recent Randomized Controlled TrialsDocument8 pagesLevosimendan in The Light of The Results of Recent Randomized Controlled TrialsMoises Agustin Preciado AlvarezNo ratings yet
- Psychiatric Comorbidities in Epilepsy PatientsDocument24 pagesPsychiatric Comorbidities in Epilepsy PatientsSueNo ratings yet
- Interacciones Farmacologicas de Los Farmacos Utilizados en AnestesiaDocument12 pagesInteracciones Farmacologicas de Los Farmacos Utilizados en AnestesiaPaulina BarragánNo ratings yet
- Okuyama Et Al. 2015 - Statins Stimulate Atherosclerosis and Heart Failure, Pharmacological MechanismsDocument11 pagesOkuyama Et Al. 2015 - Statins Stimulate Atherosclerosis and Heart Failure, Pharmacological MechanismsAlbert CalvetNo ratings yet
- Oxford Medicine Online: Biomarkers in Acute Heart FailureDocument33 pagesOxford Medicine Online: Biomarkers in Acute Heart Failuremarie saulNo ratings yet
- Pharmacokinetic Changes in Congestive Heart FailurDocument9 pagesPharmacokinetic Changes in Congestive Heart FailurKami EunNo ratings yet
- Ijpvm 2 64Document9 pagesIjpvm 2 64Soraya DiliwiyaniNo ratings yet
- PP 2015052815410826Document13 pagesPP 2015052815410826Lidia Lilywandwi SimatupangNo ratings yet
- Beneficial Effect of Cyclosporine A On Traumatic Hemorrhagic ShockDocument12 pagesBeneficial Effect of Cyclosporine A On Traumatic Hemorrhagic ShockJoecoNo ratings yet
- Sex Dependent Changes in Physical, Mental, And.67Document8 pagesSex Dependent Changes in Physical, Mental, And.67maria fernanda bahena gomezNo ratings yet
- Analgesic constant rate infusions in dogs and catsDocument7 pagesAnalgesic constant rate infusions in dogs and catsOlga Lucia Duque QuijanoNo ratings yet
- Efficacy and Safety of Amlodipine Versus Captopril and Their Combination Inhypertensive Urgency A Randomized Controlled Trial 2329 9126 1000274 PDFDocument7 pagesEfficacy and Safety of Amlodipine Versus Captopril and Their Combination Inhypertensive Urgency A Randomized Controlled Trial 2329 9126 1000274 PDFMaya sariNo ratings yet
- Antiplatelet DrugsDocument5 pagesAntiplatelet DrugsAhmad DzakyNo ratings yet
- Comparison of The Haemodynamic Effects and Seizure Activity During Modified ECT With Thiopentone and Propofol Used As Inducing AgentsDocument15 pagesComparison of The Haemodynamic Effects and Seizure Activity During Modified ECT With Thiopentone and Propofol Used As Inducing AgentsIOSR Journal of PharmacyNo ratings yet
- Antioxidant Activity of Linalool in Patients With CTSDocument6 pagesAntioxidant Activity of Linalool in Patients With CTSIn Yen ThengNo ratings yet
- Opa 1Document7 pagesOpa 1Wakum LNo ratings yet
- Cardiac Rehabilitation and Endothelial Function: Clinical MedicineDocument15 pagesCardiac Rehabilitation and Endothelial Function: Clinical Medicinetri windartiNo ratings yet
- Guidelines For The Diagnosis, Treatment and Prevention of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2009)Document24 pagesGuidelines For The Diagnosis, Treatment and Prevention of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2009)Carlos JohnsonNo ratings yet
- Ranolazine: A Novel Antianginal Compound: Ua'Ica 'Document1 pageRanolazine: A Novel Antianginal Compound: Ua'Ica 'belaginaNo ratings yet
- Antiplatelet Agents For Stroke PreventionDocument13 pagesAntiplatelet Agents For Stroke PreventionYanthie Moe MunkNo ratings yet
- Journal 4 - Management of Traumatic Brain Injury A Narrative Review of Current EvidenceDocument11 pagesJournal 4 - Management of Traumatic Brain Injury A Narrative Review of Current EvidenceNatalindah Jokiem Woecandra T. D.No ratings yet
- Review Article: Elevated Blood Pressure in The Acute Phase of Stroke and The Role of Angiotensin Receptor BlockersDocument8 pagesReview Article: Elevated Blood Pressure in The Acute Phase of Stroke and The Role of Angiotensin Receptor BlockersPatrick RamosNo ratings yet
- Hyperlipidemia in Stroke Pathobiology and Therapy: Insights and PerspectivesDocument6 pagesHyperlipidemia in Stroke Pathobiology and Therapy: Insights and Perspectivesputri aprilliaNo ratings yet
- Guide to using a polypill for cardiovascular risk reductionDocument12 pagesGuide to using a polypill for cardiovascular risk reductionjordiNo ratings yet
- 12 JMSCRDocument6 pages12 JMSCRArdianNo ratings yet
- Graduation Projects of 5 Year Students 2018/2019 1-Nameer Afaat Nassar Title: Approaches For The Treatment of Neuropathic PainDocument3 pagesGraduation Projects of 5 Year Students 2018/2019 1-Nameer Afaat Nassar Title: Approaches For The Treatment of Neuropathic PainaillNo ratings yet
- ASCOT TrialDocument8 pagesASCOT TrialMigs MedinaNo ratings yet
- Estatina en Cardio Nov 05Document9 pagesEstatina en Cardio Nov 05ja30jd15ve15an22No ratings yet
- Novel-Antiplatelet Therapies For Atherothrombotic Diseases: K.malleswari, D.Rama Bramha Reddy, A.Karthikeya SharmaDocument8 pagesNovel-Antiplatelet Therapies For Atherothrombotic Diseases: K.malleswari, D.Rama Bramha Reddy, A.Karthikeya Sharma9493.karthikNo ratings yet
- Triptans and Migraine: Advances in Use, Administration, Formulation, and DevelopmentDocument35 pagesTriptans and Migraine: Advances in Use, Administration, Formulation, and DevelopmentMartin GiraudoNo ratings yet
- Comparative Study To Evaluate Efficacy & Cost Effectiveness of Olmesartan Versus Telmisartan, in Patients of Stage I HypertensionDocument9 pagesComparative Study To Evaluate Efficacy & Cost Effectiveness of Olmesartan Versus Telmisartan, in Patients of Stage I Hypertensiondini hanifaNo ratings yet
- Assessment of Quality of Life in A Double-Blind, Randomized Clinical Trial of Imidapril and Captopril For Hypertensive Chinese in TaiwanDocument7 pagesAssessment of Quality of Life in A Double-Blind, Randomized Clinical Trial of Imidapril and Captopril For Hypertensive Chinese in TaiwanSherllen ChandraNo ratings yet
- Pharmacology & TherapeuticsDocument20 pagesPharmacology & TherapeuticsSantiago PilataxiNo ratings yet
- Intoxicacion Por Betabloqueadores ToxicologyDocument42 pagesIntoxicacion Por Betabloqueadores ToxicologyIza ÁlvarezNo ratings yet
- Latelet Function Testing Guided Antiplatelet Therapy: Ekaterina Lenk, Michael SpannaglDocument7 pagesLatelet Function Testing Guided Antiplatelet Therapy: Ekaterina Lenk, Michael SpannaglViona PrasetyoNo ratings yet
- Role of "Old" Pharmacological Agents in The Treatment of Cushing's SyndromeDocument9 pagesRole of "Old" Pharmacological Agents in The Treatment of Cushing's SyndromeErnesto Castañeda VargasNo ratings yet
- How Does Empagliflozin Improve Arterial Stiffness in Patients With Type 2 Diabetes Mellitus - Sub Analysis of A Clinical TrialDocument12 pagesHow Does Empagliflozin Improve Arterial Stiffness in Patients With Type 2 Diabetes Mellitus - Sub Analysis of A Clinical TrialMarshall ThompsonNo ratings yet
- JurnalDocument5 pagesJurnalkadekNo ratings yet
- 10 1177@1074248418769054Document11 pages10 1177@1074248418769054Bidhur Chakma 1935371673No ratings yet
- RESPIRATORY CASE - Sol - GargantielDocument4 pagesRESPIRATORY CASE - Sol - GargantielMaryglen GargantielNo ratings yet
- Ni Hms 604442Document26 pagesNi Hms 604442Gaby ValenzuelaNo ratings yet
- Antiplatelet Therapy in Older Adults With Non-ST-Segment Elevation Acute Coronary Syndrome: Considering Risks and BenefitsDocument6 pagesAntiplatelet Therapy in Older Adults With Non-ST-Segment Elevation Acute Coronary Syndrome: Considering Risks and BenefitsJicko Street HooligansNo ratings yet
- Medi 100 E23805Document5 pagesMedi 100 E23805viva dialysisNo ratings yet
- Cardiovascular Risk in Clopidogrel-Treated Patients According To Cytochrome P450 2C19 2 Loss-of-Function Allele or Proton Pump Inhibitor CoadministrationDocument10 pagesCardiovascular Risk in Clopidogrel-Treated Patients According To Cytochrome P450 2C19 2 Loss-of-Function Allele or Proton Pump Inhibitor CoadministrationVenansius ReinaldiNo ratings yet
- AntiagreganteDocument19 pagesAntiagregantecNo ratings yet
- Rezitriptan in MigraneDocument19 pagesRezitriptan in MigraneGurdeep SinghNo ratings yet
- Ni 04058Document3 pagesNi 04058Febyan AbotNo ratings yet
- Cea AmlodipineDocument6 pagesCea AmlodipineM UlfahNo ratings yet
- 24 RV16006Document14 pages24 RV16006RhenalNo ratings yet
- Efficacy and Safety of Amlodipine Versus Captopril and Their Combination Inhypertensive Urgency A Randomized Controlled Trial 2329 9126 1000274Document7 pagesEfficacy and Safety of Amlodipine Versus Captopril and Their Combination Inhypertensive Urgency A Randomized Controlled Trial 2329 9126 1000274Laras OktavianiNo ratings yet
- 2.2 X 2 Feet Macgd3 Cake DesignDocument1 page2.2 X 2 Feet Macgd3 Cake DesignLinto JohnNo ratings yet
- Same Eliminates Free Radicals, Protects LiverDocument1 pageSame Eliminates Free Radicals, Protects LiverLinto JohnNo ratings yet
- Pathophysiology and Therapy of Myocardial Ischaemia/reperfusion SyndromeDocument14 pagesPathophysiology and Therapy of Myocardial Ischaemia/reperfusion SyndromeLinto JohnNo ratings yet
- 1 S-Adenosyl-L-methionine Synthetase and Phospholipid Methyltransferase Are Inhibited in Human Cirrhosis. Hepatology 1988 8:65-8Document2 pages1 S-Adenosyl-L-methionine Synthetase and Phospholipid Methyltransferase Are Inhibited in Human Cirrhosis. Hepatology 1988 8:65-8Linto JohnNo ratings yet
- Evidences On SAMe in Liver DiseasesDocument1 pageEvidences On SAMe in Liver DiseasesLinto JohnNo ratings yet
- Neutrophil Stunning by Metoprolol Reduces Infarct Size: ArticleDocument15 pagesNeutrophil Stunning by Metoprolol Reduces Infarct Size: ArticleLinto JohnNo ratings yet
- Evolving Therapies For Myocardial Ischemia-Reperfusion InjuryDocument18 pagesEvolving Therapies For Myocardial Ischemia-Reperfusion InjuryLinto JohnNo ratings yet
- HF GuidelinesDocument76 pagesHF GuidelinesLinto JohnNo ratings yet
- Final Evolution in Respiratory Medicine - Copy1Document49 pagesFinal Evolution in Respiratory Medicine - Copy1Linto JohnNo ratings yet
- Exacerbations GoldDocument10 pagesExacerbations GoldLinto JohnNo ratings yet
- Exacerbations GoldDocument10 pagesExacerbations GoldLinto JohnNo ratings yet
- GINA Flare UpsDocument15 pagesGINA Flare UpsLinto JohnNo ratings yet
- Restenosis After Coronary and Peripheral Intervention: Efficacy and Clinical Impact of CilostazolDocument8 pagesRestenosis After Coronary and Peripheral Intervention: Efficacy and Clinical Impact of CilostazolLinto JohnNo ratings yet
- Clopidogrel Versus Ticagrelor o Prasugrel en Pacientes de 70 Años o Más Con Síndrome Coronario Agudo Sin Elevación Del Segmento ST (POPular AGE)Document8 pagesClopidogrel Versus Ticagrelor o Prasugrel en Pacientes de 70 Años o Más Con Síndrome Coronario Agudo Sin Elevación Del Segmento ST (POPular AGE)Frank Antony Arizabal GaldosNo ratings yet
- A New Strategy in Reliever Therapy Budesonide/Formoterol Maintenance PlusDocument13 pagesA New Strategy in Reliever Therapy Budesonide/Formoterol Maintenance PlusLinto JohnNo ratings yet
- Airway Inflammation Induced SputumDocument2 pagesAirway Inflammation Induced SputumLinto JohnNo ratings yet
- Viral Infection in Community-Acquired Pneumonia: A Systematic Review and Meta-AnalysisDocument11 pagesViral Infection in Community-Acquired Pneumonia: A Systematic Review and Meta-AnalysisLinto JohnNo ratings yet
- Air Pollution A Big Killer in India: Source: World Health OrganisationDocument1 pageAir Pollution A Big Killer in India: Source: World Health OrganisationLinto JohnNo ratings yet
- StatusasthmaticusDocument40 pagesStatusasthmaticusLinto JohnNo ratings yet
- Pharma MarketingDocument167 pagesPharma MarketingLinto JohnNo ratings yet
- What Is CopdDocument4 pagesWhat Is CopdLinto JohnNo ratings yet
- For Uncontrolled Asthma Despite ICS: Tiotropium Add-On TXDocument1 pageFor Uncontrolled Asthma Despite ICS: Tiotropium Add-On TXLinto JohnNo ratings yet
- Coming SoonDocument1 pageComing SoonLinto JohnNo ratings yet
- Coming SoonDocument1 pageComing SoonLinto JohnNo ratings yet
- Coming SoonDocument1 pageComing SoonLinto JohnNo ratings yet
- Recent Advances in Asthma ManagementDocument6 pagesRecent Advances in Asthma ManagementLinto JohnNo ratings yet
- Zero Day REspi Test PaperDocument3 pagesZero Day REspi Test PaperLinto JohnNo ratings yet
- AutohalerDocument51 pagesAutohalerLinto JohnNo ratings yet
- Potential Drug That Could Help Treat Cystic Fibrosis Identified by ResearchersDocument2 pagesPotential Drug That Could Help Treat Cystic Fibrosis Identified by ResearchersLinto JohnNo ratings yet
- Insurance Fraud PPT (Final)Document30 pagesInsurance Fraud PPT (Final)Gaurav Savlani83% (6)
- Central Pain Syndrome - Pathophysiol., Diag., Mgmt. - S. Canavero, Et. Al., (Cambridge, 2006) WW PDFDocument398 pagesCentral Pain Syndrome - Pathophysiol., Diag., Mgmt. - S. Canavero, Et. Al., (Cambridge, 2006) WW PDFRomeo-Remus RaffaiNo ratings yet
- Prevalence of GERD in Dyspepsia PatientsDocument6 pagesPrevalence of GERD in Dyspepsia PatientsAbrar TaraNo ratings yet
- Nursing Care Plans for Respiratory and Circulatory IssuesDocument5 pagesNursing Care Plans for Respiratory and Circulatory IssuesApryll Kristin Villaluna ZafeNo ratings yet
- Berklee Intro Music Therapy PDFDocument17 pagesBerklee Intro Music Therapy PDFTheodore VaillantNo ratings yet
- SSIPDocument4 pagesSSIPGlenn Clemente100% (2)
- A Comparative Study of The Efficacy of Cedarwood Oil, Coconut Oil and Dish Wash Liquid As Alternatives To Xylene As Deparaffinizing AgentsDocument98 pagesA Comparative Study of The Efficacy of Cedarwood Oil, Coconut Oil and Dish Wash Liquid As Alternatives To Xylene As Deparaffinizing AgentszzzzNo ratings yet
- Tile Setting NC II Training RegulationsDocument67 pagesTile Setting NC II Training RegulationsRTC Zamboanga100% (1)
- Nursing assessment diagnosis interventions rationale evaluationDocument3 pagesNursing assessment diagnosis interventions rationale evaluationanimesh pandaNo ratings yet
- 100 Item Exam On Fundamentals of Nursing - Pulse - Blood Pressure PDFDocument12 pages100 Item Exam On Fundamentals of Nursing - Pulse - Blood Pressure PDFJawad AkbarNo ratings yet
- Ultrasound-Guided Lumbar Central Neuraxial Block 2016Document8 pagesUltrasound-Guided Lumbar Central Neuraxial Block 2016drkis20100% (1)
- Chapter 1 2 3Document77 pagesChapter 1 2 3Ferissa MohammadNo ratings yet
- 3-Women Athletes Knee Injuries - 2005Document9 pages3-Women Athletes Knee Injuries - 2005Fernanda CarvalhoNo ratings yet
- Pulmonary TB RadiologyDocument45 pagesPulmonary TB RadiologyArina Windri RivartiNo ratings yet
- Pathological Urine ConstituentsDocument22 pagesPathological Urine Constituentsmanni1001100% (3)
- AOTA Statement On Role of OT in NICUDocument9 pagesAOTA Statement On Role of OT in NICUMapi RuizNo ratings yet
- Global Urology Devices MarketDocument14 pagesGlobal Urology Devices MarketNamrataNo ratings yet
- A Critical Review of The Effect of Working Conditions On Employee PerformanceDocument11 pagesA Critical Review of The Effect of Working Conditions On Employee PerformanceStephanie Bacunawa0% (1)
- Thomas Foot ReflexologyDocument112 pagesThomas Foot ReflexologySa MiNo ratings yet
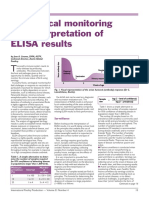
- Serological Monitoring by ELISADocument3 pagesSerological Monitoring by ELISAreza tavayef100% (1)
- Hospital Self Assement ToolkitDocument28 pagesHospital Self Assement ToolkitNidhi VijanNo ratings yet
- Grief & Grieving ProcessDocument39 pagesGrief & Grieving Processelmerconde100% (4)
- Ulcerative ColitisDocument12 pagesUlcerative Colitisthap87No ratings yet
- Cysts of The JawsDocument75 pagesCysts of The JawsSwetha KaripineniNo ratings yet
- 3 MDRRMC SampleDocument57 pages3 MDRRMC SampleMakoy Salonga100% (2)
- Care of Patient With Respiratory DisordersDocument35 pagesCare of Patient With Respiratory Disorderskriiteeabns100% (1)
- Child Neglect in Rich Nations - Sylvia HewlettDocument70 pagesChild Neglect in Rich Nations - Sylvia HewlettMarko KrstićNo ratings yet
- Unit 1-Omd553-Telehealth TechnologyDocument53 pagesUnit 1-Omd553-Telehealth TechnologyjgjeslinNo ratings yet
- Appendix7 I-131Document4 pagesAppendix7 I-131Crizzz001No ratings yet
- Hygiene Rules For Hotel Kitchen and Food Production StaffDocument3 pagesHygiene Rules For Hotel Kitchen and Food Production Staffvishnu nairNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)