You might also like
- Potential and Limitations of Orthodontic Biomechanics RecognizingDocument9 pagesPotential and Limitations of Orthodontic Biomechanics RecognizingLisbethNo ratings yet
- The Scope and Limitation of Fixed AppliancesDocument4 pagesThe Scope and Limitation of Fixed AppliancesAthirah AzizNo ratings yet
- Myth in OrthoDocument7 pagesMyth in Orthosurendra334No ratings yet
- Biological Basis For Orthodontic Tooth MovementDocument31 pagesBiological Basis For Orthodontic Tooth Movementindumathi thevanNo ratings yet
- Risk and Limitations of Orthodontic TreatmentDocument41 pagesRisk and Limitations of Orthodontic TreatmentAjay ChhetriNo ratings yet
- Modern Begg - / Orthodontic Courses by Indian Dental AcademyDocument54 pagesModern Begg - / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Cellular, Molecular, and Tissue-Level Reactions To Orthodontic ForceDocument32 pagesCellular, Molecular, and Tissue-Level Reactions To Orthodontic Forcecarlina_the_bestNo ratings yet
- A Review of Root Resorption in Orthodontics PDFDocument5 pagesA Review of Root Resorption in Orthodontics PDFRahulLife'sNo ratings yet
- Ricketts TriadDocument23 pagesRicketts TriadSonu RajuNo ratings yet
- Moving The TeethDocument117 pagesMoving The TeethThirunavukkarasu Srinivasan100% (2)
- Intrusion MechanicsDocument31 pagesIntrusion Mechanicsaa bbNo ratings yet
- Impacted Maxillary Canines-A Review. - American Journal of Orthodontics and Dentofacial Orthopedics, 101-159, 1992 PDFDocument13 pagesImpacted Maxillary Canines-A Review. - American Journal of Orthodontics and Dentofacial Orthopedics, 101-159, 1992 PDFPia ContrerasNo ratings yet
- Advances in Biology of Orthodontic Tooth Movement - A ReviewDocument10 pagesAdvances in Biology of Orthodontic Tooth Movement - A ReviewMarwan AlareqiNo ratings yet
- Made By: Sumera Hashmani Roll Number:38 Jabbar Ahmed Roll Number: 50Document33 pagesMade By: Sumera Hashmani Roll Number:38 Jabbar Ahmed Roll Number: 50Maira HassanNo ratings yet
- ArchwiresDocument14 pagesArchwiresBhavikPatelNo ratings yet
- Biomechanics in Orthodontics - A Review (Part 1) IJODODocument11 pagesBiomechanics in Orthodontics - A Review (Part 1) IJODOPranshu MathurNo ratings yet
- Tads 1Document6 pagesTads 1travolta0No ratings yet
- WiresDocument140 pagesWiresRushabh ShahNo ratings yet
- Principles of The Alexander DisciplineDocument5 pagesPrinciples of The Alexander DisciplineSarah Fauzia SiregarNo ratings yet
- Mode of Action of Functional Appliances / Orthodontic Courses by Indian Dental AcademyDocument116 pagesMode of Action of Functional Appliances / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Fixed Functional ApplianceDocument71 pagesFixed Functional AppliancekpNo ratings yet
- Ortho Case ReportDocument6 pagesOrtho Case ReportAlex Adille OgaoNo ratings yet
- Functional Appliances: Click To Edit Master Subtitle Style Dr. Rashid MahmoodDocument150 pagesFunctional Appliances: Click To Edit Master Subtitle Style Dr. Rashid MahmoodZawara MariamNo ratings yet
- Basic Principles of GrowthDocument29 pagesBasic Principles of GrowthMohsin HabibNo ratings yet
- Torque in OrthodonticsDocument115 pagesTorque in OrthodonticsRohini TondaNo ratings yet
- Evolution of Treatment Mechanics and Contemporary Appliance Design in Orthodontics: A 40-Year PerspectiveDocument9 pagesEvolution of Treatment Mechanics and Contemporary Appliance Design in Orthodontics: A 40-Year PerspectiveBeatriz ChilenoNo ratings yet
- Condylar CartilageDocument11 pagesCondylar CartilageMahesh kumarNo ratings yet
- Malocclusion OrthoDocument79 pagesMalocclusion OrthoFourthMolar.com100% (2)
- Equilibrium Theory of Tooth Position IIDocument12 pagesEquilibrium Theory of Tooth Position IILIZETH NATHALIA TOLOZA OCHOANo ratings yet
- Preventive OrthodonticDocument19 pagesPreventive OrthodonticNada EmadNo ratings yet
- Bomechancs in OrthodotnicsDocument74 pagesBomechancs in OrthodotnicsheycoolalexNo ratings yet
- Behavior OrthoDocument96 pagesBehavior OrthoarshabharataNo ratings yet
- American Journal QF Orthodontics: Facial Types Associated With Class II MalocclusionsDocument18 pagesAmerican Journal QF Orthodontics: Facial Types Associated With Class II MalocclusionsKhyati Gupta100% (1)
- Soft Tissue Analysis: Dr. Ayushi Toley PG Ist YearDocument70 pagesSoft Tissue Analysis: Dr. Ayushi Toley PG Ist YearAyushi ToleyNo ratings yet
- Mechanics in OccDocument29 pagesMechanics in OccDrAla MohamedNo ratings yet
- Retention and Relapse SeminarDocument51 pagesRetention and Relapse SeminarShipra SehgalNo ratings yet
- ISSN 2347-5579: 0.018" Versus 0.022" Bracket Slot Systems in Orthodontics: A ReviewDocument4 pagesISSN 2347-5579: 0.018" Versus 0.022" Bracket Slot Systems in Orthodontics: A ReviewRahulLife's100% (1)
- Rapid MaxillaryDocument24 pagesRapid MaxillaryDon George GeojanNo ratings yet
- Anterior and Canine RetractionDocument10 pagesAnterior and Canine RetractionLisbethNo ratings yet
- 21 178 1 PBDocument7 pages21 178 1 PBClinica Dental AdvanceNo ratings yet
- The Anchorage Bend in The Begg TechniqueDocument7 pagesThe Anchorage Bend in The Begg TechniqueSyed Mohammad Osama AhsanNo ratings yet
- Digital Photography in OrthodonDocument48 pagesDigital Photography in OrthodonSrinivasan BoovaraghavanNo ratings yet
- Theories of GrowthDocument137 pagesTheories of GrowthYuvashreeNo ratings yet
- WittsDocument39 pagesWittsAya ElsayedNo ratings yet
- Beta Angle 2003Document6 pagesBeta Angle 2003surendra334No ratings yet
- Beggs TechniqueDocument24 pagesBeggs TechniqueGAURAV VARMANo ratings yet
- Extraoral Orthopaedic AppliancesDocument59 pagesExtraoral Orthopaedic AppliancesAmatullahsadiyaNo ratings yet
- Class III TTT OptionsDocument9 pagesClass III TTT OptionsMADANo ratings yet
- 6 Biomechanical Basis of Extraction Space Closure - Pocket DentistryDocument5 pages6 Biomechanical Basis of Extraction Space Closure - Pocket DentistryParameswaran ManiNo ratings yet
- Fixed Functional Appliances For Treatment of Class II Malocclusions Effects and LimitationsDocument35 pagesFixed Functional Appliances For Treatment of Class II Malocclusions Effects and LimitationsAya ElsayedNo ratings yet
- Ceph HandoutDocument18 pagesCeph Handoutwaheguru13he13No ratings yet
- Catalog - 2010 Lancer OrthoDocument179 pagesCatalog - 2010 Lancer OrthoAnonymous vyzrdPNo ratings yet
- Indices PDFDocument10 pagesIndices PDFBhavikPatelNo ratings yet
- Methods of Cephalometric Superimposition - A ReviewDocument4 pagesMethods of Cephalometric Superimposition - A ReviewAniket PotnisNo ratings yet
- Orthodontic Biomechanics: Treatment Of Complex Cases Using Clear AlignerFrom EverandOrthodontic Biomechanics: Treatment Of Complex Cases Using Clear AlignerNo ratings yet
- Healers Versus Stealers: How to Outsmart the Thief in Your Dental PracticeFrom EverandHealers Versus Stealers: How to Outsmart the Thief in Your Dental PracticeNo ratings yet
- 7 RetainerinorthodonticsDocument6 pages7 RetainerinorthodonticsramadanNo ratings yet
- 113 217 1 PB PDFDocument6 pages113 217 1 PB PDFdup11No ratings yet
- Retantion and Relapse by DR Tamanna HabibDocument32 pagesRetantion and Relapse by DR Tamanna HabibTamanna HabibNo ratings yet
- Immediate Denture A ReviewDocument5 pagesImmediate Denture A ReviewAswathi RaghuthamanNo ratings yet
- Support in Complete DentureDocument30 pagesSupport in Complete DentureSahana Rangarajan100% (2)
- Support in Complete DentureDocument16 pagesSupport in Complete DentureSahana RangarajanNo ratings yet
- Dynamic Navigation in Dental Implantology: The Influence of Surgical Experience On Implant Placement Accuracy and Operating Time. An in Vitro StudyDocument9 pagesDynamic Navigation in Dental Implantology: The Influence of Surgical Experience On Implant Placement Accuracy and Operating Time. An in Vitro StudySahana RangarajanNo ratings yet
- Mandibular MovementDocument56 pagesMandibular MovementSahana RangarajanNo ratings yet
- Different Types of Tooth PreparationDocument56 pagesDifferent Types of Tooth PreparationSahana Rangarajan100% (1)
- Finishing and Polishing Agents: - Presented by DR Arpita DuttaDocument89 pagesFinishing and Polishing Agents: - Presented by DR Arpita DuttaSahana RangarajanNo ratings yet
- Factors Affecting Shade of All Ceramic Restorations - A Literature ReviewDocument8 pagesFactors Affecting Shade of All Ceramic Restorations - A Literature ReviewSahana RangarajanNo ratings yet
- A Hollow Bulb Obturator For Maxillary Resection in A Completely Edentulous PatientDocument6 pagesA Hollow Bulb Obturator For Maxillary Resection in A Completely Edentulous PatientSahana RangarajanNo ratings yet
- Clinical Report Rehabilitation of Maxillary Surgical Defect With A Cast Partial Denture ObturatorDocument4 pagesClinical Report Rehabilitation of Maxillary Surgical Defect With A Cast Partial Denture ObturatorSahana RangarajanNo ratings yet
- Fulltext - Jda v5 Id1107Document3 pagesFulltext - Jda v5 Id1107Sahana RangarajanNo ratings yet
- 6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothDocument6 pages6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothSahana RangarajanNo ratings yet
- Long-Term Follow-Up of Maxillary Fixed Retention: Survival Rate and Periodontal HealthDocument7 pagesLong-Term Follow-Up of Maxillary Fixed Retention: Survival Rate and Periodontal HealthSahana RangarajanNo ratings yet
- 7 Shreeprada Dash IJPHRDDecember 2018 IssueDocument7 pages7 Shreeprada Dash IJPHRDDecember 2018 IssueSahana RangarajanNo ratings yet
- Elegant Galaxy Background Breakthrough by SlidesgoDocument48 pagesElegant Galaxy Background Breakthrough by SlidesgoSahana RangarajanNo ratings yet
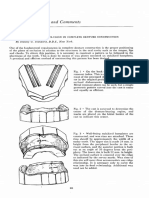
- Cases and Comments: by Stanley G. Standard, D.D.S., New YorkDocument3 pagesCases and Comments: by Stanley G. Standard, D.D.S., New YorkSahana RangarajanNo ratings yet
- 3D Printing Industry Roadmap - India (Aerospace) Summit DocumentDocument19 pages3D Printing Industry Roadmap - India (Aerospace) Summit DocumentSahana RangarajanNo ratings yet
- Review: Types of Finish Lines or Gingival Margins Intooth PreparationDocument6 pagesReview: Types of Finish Lines or Gingival Margins Intooth PreparationSahana RangarajanNo ratings yet
- Prosthodontics Horizontal Jaw Relation: Dr. Firas AbdulameerDocument6 pagesProsthodontics Horizontal Jaw Relation: Dr. Firas AbdulameerSahana RangarajanNo ratings yet
- Mouth Guards in Dentistry-A Review: September 2018Document6 pagesMouth Guards in Dentistry-A Review: September 2018Sahana RangarajanNo ratings yet
- Significance of Facebow For Dental RestorationsDocument5 pagesSignificance of Facebow For Dental RestorationsSahana RangarajanNo ratings yet
- Sauser 1957Document9 pagesSauser 1957Sahana RangarajanNo ratings yet
- Occlusion in Complete DentureDocument57 pagesOcclusion in Complete DentureSahana Rangarajan100% (1)
- Gothic Arch TrachingDocument7 pagesGothic Arch TrachingSahana RangarajanNo ratings yet
- Glassman 1984Document7 pagesGlassman 1984Ashish KushwahNo ratings yet
- Treatment of Posterior Crossbite Comparing 2 Appliances: A Community-Based TrialDocument8 pagesTreatment of Posterior Crossbite Comparing 2 Appliances: A Community-Based TrialPae Anusorn AmtanonNo ratings yet
- AAPD - The Handbook of Pediatric Dentistry PDFDocument332 pagesAAPD - The Handbook of Pediatric Dentistry PDFRaissa Ica80% (10)
- (Sh2) Rapid Maxillary ExpansionDocument137 pages(Sh2) Rapid Maxillary ExpansionnivethaseshaNo ratings yet
- Treatment Timing Orthodontics in Four DimensionsDocument281 pagesTreatment Timing Orthodontics in Four DimensionsLobo GrisNo ratings yet
- Dental Notes PDFDocument144 pagesDental Notes PDFAlan Tahsin100% (3)
- Advantages of Serial ExtractionDocument4 pagesAdvantages of Serial ExtractionsimbonaNo ratings yet
- DownloadDocument12 pagesDownloadRodrigo PontesNo ratings yet
- Scientific Posters v2Document217 pagesScientific Posters v2Cernei Eduard RaduNo ratings yet
- 1000mcq SOLUTIONSDocument198 pages1000mcq SOLUTIONSTrivedi VE100% (1)
- The Science Behind The System: Clinical Abstracts, Volume 2Document8 pagesThe Science Behind The System: Clinical Abstracts, Volume 2dana40018256No ratings yet
- Policy On PacifiersDocument4 pagesPolicy On PacifiersمعتزباللهNo ratings yet
- Serial ExtractionDocument9 pagesSerial ExtractionFarheen MahmoodaNo ratings yet
- Logbook Scen 5 PedoDocument4 pagesLogbook Scen 5 PedoQutrunnada MahaninNo ratings yet
- 15 - Digital Workflow For Mini-implant-Assisted Rapid Palatal Expander Fabrication-A Case ReportDocument13 pages15 - Digital Workflow For Mini-implant-Assisted Rapid Palatal Expander Fabrication-A Case ReportMariana SantosNo ratings yet
- Pedo QsDocument13 pagesPedo QsGaYda'a Kana'anNo ratings yet
- Crossbite: ClassificationDocument8 pagesCrossbite: ClassificationYousif Abdulla100% (1)
- Journal of Cranio-Maxillo-Facial Surgery: Mohammad Zandi, Amirfarhang Miresmaeili, Ali HeidariDocument6 pagesJournal of Cranio-Maxillo-Facial Surgery: Mohammad Zandi, Amirfarhang Miresmaeili, Ali HeidariYeraldin EspañaNo ratings yet
- March Rqs COMPILED BY DR. STRANGEDocument89 pagesMarch Rqs COMPILED BY DR. STRANGEghassan100% (1)
- Malocclusion in Saudi Arabia: A Scoping ReviewDocument5 pagesMalocclusion in Saudi Arabia: A Scoping ReviewRati Ramayani AbidinNo ratings yet
- Removable Appliances Author DR Lamis Khidher MohammedDocument11 pagesRemovable Appliances Author DR Lamis Khidher MohammedRuxandra FitaNo ratings yet
- Interceptive OrthodonticsDocument27 pagesInterceptive OrthodonticsDivya Shrivastava100% (1)
- Long-Term Follow-Up of A Patient With Achondroplasia Treated With An Orthodontic ApproachDocument11 pagesLong-Term Follow-Up of A Patient With Achondroplasia Treated With An Orthodontic ApproachThuyNo ratings yet
- CJQ 182Document6 pagesCJQ 182habeebNo ratings yet
- Esthetic Optimization of Surgical-Orthodontic TreatmentDocument22 pagesEsthetic Optimization of Surgical-Orthodontic TreatmentumadeviNo ratings yet
- Noel Montinaro 2020 Modified SEC III ProtocolDocument6 pagesNoel Montinaro 2020 Modified SEC III Protocolsolodont1No ratings yet
- Classification of Malocclusion FinalDocument67 pagesClassification of Malocclusion FinalRaj SinghNo ratings yet
- Oral Habits - Thumb SuckingDocument18 pagesOral Habits - Thumb SuckingSiddharthak SangwanNo ratings yet
- Role of Orthodontists in The Management of Cleft LipDocument2 pagesRole of Orthodontists in The Management of Cleft LipMd Nurul IslamNo ratings yet
- Aetiology, Diagnosis and Treatment of Posterior Cross-Bites in The Primary DentitionDocument12 pagesAetiology, Diagnosis and Treatment of Posterior Cross-Bites in The Primary DentitionARIANA AMARILES BAENANo ratings yet