You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Chronic-Cholecystitis-and-Metastatic-Breast-CA FinalDocument3 pagesChronic-Cholecystitis-and-Metastatic-Breast-CA FinalRishi Du AgbugayNo ratings yet
- Cagayan State University College of Medicine Carig Campus, Tuguegarao City Surgery WardDocument7 pagesCagayan State University College of Medicine Carig Campus, Tuguegarao City Surgery WardRishi Du AgbugayNo ratings yet
- Clinthera CaseDocument7 pagesClinthera CaseRishi Du AgbugayNo ratings yet
- (PEDIA II) 2.04 Pediatric Dermatology - AngelesDocument16 pages(PEDIA II) 2.04 Pediatric Dermatology - AngelesRishi Du AgbugayNo ratings yet
- Pedia Case 1 Dengue 1Document9 pagesPedia Case 1 Dengue 1Rishi Du Agbugay100% (1)
- Psychiatric Case Presentation: Praveenrajkumar Csu Junior InternDocument33 pagesPsychiatric Case Presentation: Praveenrajkumar Csu Junior InternRishi Du AgbugayNo ratings yet
- (PEDIA II) 1.01 Neonatology I - SalazarDocument23 pages(PEDIA II) 1.01 Neonatology I - SalazarRishi Du AgbugayNo ratings yet
- The Effectiveness of Yacon (Smallanthus Sonchifolius Tuber Extract As A Blood-Glucose Lowering SweeterDocument12 pagesThe Effectiveness of Yacon (Smallanthus Sonchifolius Tuber Extract As A Blood-Glucose Lowering SweeterRishi Du AgbugayNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Common Diseases of The Reproductive SystemDocument5 pagesCommon Diseases of The Reproductive SystemIrish Lara ARCENo ratings yet
- Ovarian Dysgerminomas Pathology Overview of Ovarian DysgerminomasDocument7 pagesOvarian Dysgerminomas Pathology Overview of Ovarian DysgerminomasDevi SyamNo ratings yet
- Anatomy of The Male Reproductive SystemDocument70 pagesAnatomy of The Male Reproductive SystemDaniel HikaNo ratings yet
- A Case of PriapismDocument2 pagesA Case of Priapismsarina sateiNo ratings yet
- Ovarian Torsion in Pregnancy A Case ReportDocument3 pagesOvarian Torsion in Pregnancy A Case ReportCakraEkkyNo ratings yet
- Euthenics ModuleDocument4 pagesEuthenics ModuleHanna AsmadNo ratings yet
- INFERTILITYDocument20 pagesINFERTILITYKathleen FrugalidadNo ratings yet
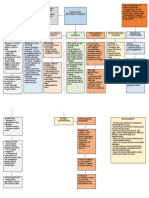
- Concept-Map ESCULTORDocument2 pagesConcept-Map ESCULTORDaniela Claire FranciscoNo ratings yet
- Science 5 - 2ND QuarterDocument4 pagesScience 5 - 2ND QuarterRica VillanuevaNo ratings yet
- Artificial Insemination ProcedureDocument9 pagesArtificial Insemination ProcedureJyotiNo ratings yet
- Year 8 Science OverviewDocument4 pagesYear 8 Science Overviewapi-3137245670% (1)
- Obstetrics and GynaecologyDocument43 pagesObstetrics and Gynaecologylisserrano100% (1)
- Pro CyclesDocument7 pagesPro Cyclestselentisharris15867% (3)
- Male CircumcisionDocument17 pagesMale CircumcisionJoannaMaeVillamorNo ratings yet
- Cervical CancerDocument15 pagesCervical CancerMahen BoralessaNo ratings yet
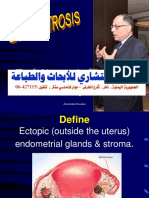
- Endometriosis 140727182255 Phpapp01Document182 pagesEndometriosis 140727182255 Phpapp01bmhsh100% (1)
- Anatomy & Physiology (Chapter 19 - Reproductive System)Document30 pagesAnatomy & Physiology (Chapter 19 - Reproductive System)Eduardo Niepes Jr.No ratings yet
- PBL Report 3 FixDocument24 pagesPBL Report 3 FixtiwiNo ratings yet
- Abortion: Case Presentation By: Kristianne Ysabel E. SorianoDocument22 pagesAbortion: Case Presentation By: Kristianne Ysabel E. SorianoyounggirldavidNo ratings yet
- Setting Up of IUI LabDocument23 pagesSetting Up of IUI LabSuryakant Hayatnagarkar90% (10)
- Menstrual Disorder Menstrual DisorderDocument78 pagesMenstrual Disorder Menstrual DisorderDeff HaningNo ratings yet
- Human Reproduction WorksheetDocument3 pagesHuman Reproduction WorksheetDEEBAN0% (1)
- Gynaecology MCQsDocument19 pagesGynaecology MCQssimi yNo ratings yet
- Semen Analysis: PG Resident, Department of Biochemistry, SGRRIMHS & SMI Hospital, DehradunDocument68 pagesSemen Analysis: PG Resident, Department of Biochemistry, SGRRIMHS & SMI Hospital, DehradunMarj MendezNo ratings yet
- Polip Serviks: Clinical Science SectionDocument15 pagesPolip Serviks: Clinical Science SectionnsrinanaNo ratings yet
- Assessment of The Genitourinary System: GeneralDocument2 pagesAssessment of The Genitourinary System: GeneralMaharani UtamiNo ratings yet
- Breast Shape Yoga PosesDocument4 pagesBreast Shape Yoga Posessubscribe_allNo ratings yet
- Infertility: Presented ByDocument47 pagesInfertility: Presented ByNilakshi Barik MandalNo ratings yet
- Mind Map - ContraceptivesDocument1 pageMind Map - ContraceptivesPriya DarshiniNo ratings yet
- Vgo Imp MCQDocument5 pagesVgo Imp MCQomprakash ChabarwalNo ratings yet