You might also like
- Marcel Case StudyDocument5 pagesMarcel Case StudyPrismatic Ray100% (1)
- PSYCH 505 Case Study Core FunctionsDocument8 pagesPSYCH 505 Case Study Core FunctionsHugsNo ratings yet
- SW 3020 Biopsychosocial Assessment-Final RevisedDocument18 pagesSW 3020 Biopsychosocial Assessment-Final Revisedapi-286703035No ratings yet
- Your PCM Profile® Your PCM Profile® Your PCM Profile® Your PCM Profile®Document38 pagesYour PCM Profile® Your PCM Profile® Your PCM Profile® Your PCM Profile®Florin ValentinNo ratings yet
- Wang ShuDocument7 pagesWang ShuKotha BhupendraNo ratings yet
- Cns 765 Case Study FinalDocument10 pagesCns 765 Case Study Finalapi-582911813No ratings yet
- Case Study Paper Final ValentineDocument10 pagesCase Study Paper Final Valentineapi-3166145030% (1)
- Case Conceptualization 514Document4 pagesCase Conceptualization 514Kyle RossNo ratings yet
- Running Head: Writing A Treatment Plan 1Document6 pagesRunning Head: Writing A Treatment Plan 1Angy ShoogzNo ratings yet
- Client Evaluation sw4997 Paper 2Document12 pagesClient Evaluation sw4997 Paper 2api-242943882No ratings yet
- The Prevalence of Substance Use and Other Mental Health Concerns Among American AttorneysDocument7 pagesThe Prevalence of Substance Use and Other Mental Health Concerns Among American AttorneysDavid AndreattaNo ratings yet
- BiopsychosocialDocument6 pagesBiopsychosocialapi-307244919No ratings yet
- Final Capstone PaperDocument15 pagesFinal Capstone Paperapi-478784238No ratings yet
- Comprehensive Case StudyDocument10 pagesComprehensive Case Studyapi-545708059No ratings yet
- 1 Case Formulation - BronDocument4 pages1 Case Formulation - BronallysoncaiNo ratings yet
- Treatment PlanDocument12 pagesTreatment PlanlawamandaNo ratings yet
- Mental Health Case StudyDocument10 pagesMental Health Case Studyapi-401649616No ratings yet
- Psych Case StudyDocument10 pagesPsych Case Studyapi-455759072No ratings yet
- Comprehensive Case StudyDocument11 pagesComprehensive Case Studyapi-546503916No ratings yet
- Student Biopsychosocial Assessment For Client A FinalizedDocument8 pagesStudent Biopsychosocial Assessment For Client A Finalizedapi-554055276No ratings yet
- 3 - Clinical Assessment, Diagnosis, and Research MethodsDocument12 pages3 - Clinical Assessment, Diagnosis, and Research Methodsapi-3855346100% (1)
- Intake AssessmentDocument2 pagesIntake Assessmentyourzxtruly0% (1)
- Sample Case Study For DMS-IV-TRDocument6 pagesSample Case Study For DMS-IV-TRohphooeyNo ratings yet
- Psychiatric Mental Health Comprehensive Case StudyDocument12 pagesPsychiatric Mental Health Comprehensive Case Studyapi-603618331No ratings yet
- Clinical Assessment Inteview, Steps To Psychological Assessment & Expression TechniquesDocument3 pagesClinical Assessment Inteview, Steps To Psychological Assessment & Expression TechniquesAnthony Pangan100% (2)
- Case Analysis Assignment: Interpersonal and Social Rhythm TherapyDocument2 pagesCase Analysis Assignment: Interpersonal and Social Rhythm TherapyJoshua RingorNo ratings yet
- Cns 6161 Treatment Plan - WalterDocument7 pagesCns 6161 Treatment Plan - Walterapi-263972200No ratings yet
- Psych Report of RDA by Ernie GarciaDocument3 pagesPsych Report of RDA by Ernie GarciaLe Ar NieNo ratings yet
- Casemapping 7 Analyzing Goals and TX PlansDocument14 pagesCasemapping 7 Analyzing Goals and TX Plansapi-436090845No ratings yet
- Psych Case StudyDocument13 pagesPsych Case Studyapi-662201129No ratings yet
- Observations of An AA MeetingDocument2 pagesObservations of An AA MeetingKaryn Ives Kerr100% (1)
- Psychosocial Theory of SchizophreniaDocument16 pagesPsychosocial Theory of SchizophreniaJona JoyNo ratings yet
- Fundamentals To Clinical PsychologyDocument6 pagesFundamentals To Clinical PsychologySurabhi RanjanNo ratings yet
- Mental Health Case StudyDocument11 pagesMental Health Case Studyapi-546878677No ratings yet
- Case Conceptualization PaperDocument14 pagesCase Conceptualization Paperapi-554055276No ratings yet
- Case Study Development and Theoretical ExplanationDocument7 pagesCase Study Development and Theoretical ExplanationAssignmentLab.com100% (1)
- Objectives: Schizophrenia. Cause, Pathophysiology: WomenDocument11 pagesObjectives: Schizophrenia. Cause, Pathophysiology: WomenDuha B. SalimNo ratings yet
- CAGE Questionnaire For Alcohol MisuseDocument10 pagesCAGE Questionnaire For Alcohol MisuseJeremy BergerNo ratings yet
- Cognitive Behavior TherapyDocument8 pagesCognitive Behavior TherapyKerem Ali YavuzNo ratings yet
- Joshua Dodot Case StudyDocument2 pagesJoshua Dodot Case StudyJoshua Ringor100% (1)
- Marino Case StudyDocument14 pagesMarino Case Studyapi-538721860No ratings yet
- Behavioural Problem Teennager: Family Medicine SystemDocument23 pagesBehavioural Problem Teennager: Family Medicine SystemSelvi Puspa SariNo ratings yet
- Conduct Disorder Fact Sheet - K. Elise Parker PDFDocument2 pagesConduct Disorder Fact Sheet - K. Elise Parker PDFepaka02No ratings yet
- Treatment Plan ExampleDocument8 pagesTreatment Plan Exampleapi-430075910No ratings yet
- Depressive Disorders Social Isolation/Impaired Social InteractionDocument5 pagesDepressive Disorders Social Isolation/Impaired Social InteractionYannesa S. Bantilan - Balbin100% (2)
- Case StudyDocument5 pagesCase StudyDerby Febriani Sultany100% (1)
- Forensic AssessmentDocument8 pagesForensic AssessmentSinginintherain1125No ratings yet
- G CBT For DelusionDocument23 pagesG CBT For DelusionIoana DarjanNo ratings yet
- Mental Health-Case Study GDocument14 pagesMental Health-Case Study Gapi-545670336No ratings yet
- Case Study Jared Tacey Youngstown State UniversityDocument13 pagesCase Study Jared Tacey Youngstown State Universityapi-402076669100% (1)
- Drug Addict Case ReportDocument18 pagesDrug Addict Case ReportHajra Khan100% (1)
- Na ReflectionDocument6 pagesNa Reflectionapi-433710976No ratings yet
- Psychosocial Development Erik EriksonDocument2 pagesPsychosocial Development Erik EriksonA.LiyanaVNo ratings yet
- Function-Memory, Smell And: Persecutory / Paranoid Delusions - Involve TheDocument4 pagesFunction-Memory, Smell And: Persecutory / Paranoid Delusions - Involve TheMark Christian CaasiNo ratings yet
- Treatment Plan 3Document8 pagesTreatment Plan 3Kathy Lee Hornbeck KendrickNo ratings yet
- Mse 1Document27 pagesMse 1Ladybelle GototosNo ratings yet
- Attention Deficit Hyperactivity Disorder (Adhd)Document43 pagesAttention Deficit Hyperactivity Disorder (Adhd)Thevanath Gunasekaran100% (1)
- CDI Patient VersionDocument9 pagesCDI Patient VersionalotfyaNo ratings yet
- Drug Addict 13,6,2020Document16 pagesDrug Addict 13,6,2020mirha fatimaNo ratings yet
- Assignment For 29.04.2021Document20 pagesAssignment For 29.04.2021RADHIKA JAISWALNo ratings yet
- Intervention, Management of HallucinationDocument52 pagesIntervention, Management of HallucinationAshish_Singh_5126No ratings yet
- Jurnal KK 8Document5 pagesJurnal KK 8NORAZLINA BINTI MOHMAD DALI / UPMNo ratings yet
- Behavioral Change Aspects and Their Effects On Drug Abuse Counseling Training)Document14 pagesBehavioral Change Aspects and Their Effects On Drug Abuse Counseling Training)NORAZLINA BINTI MOHMAD DALI / UPMNo ratings yet
- Jurnal KK 2Document23 pagesJurnal KK 2NORAZLINA BINTI MOHMAD DALI / UPM100% (1)
- T G G I M P U: E T L B ': He Ender Ap N Alaysian Ublic Niversities Xamining He Ost OysDocument16 pagesT G G I M P U: E T L B ': He Ender Ap N Alaysian Ublic Niversities Xamining He Ost OysNORAZLINA BINTI MOHMAD DALI / UPMNo ratings yet
- Sexual: SocialDocument7 pagesSexual: SocialNORAZLINA BINTI MOHMAD DALI / UPMNo ratings yet
- The Evolving Evidence Base For Child Protection in Chinese SocietiesDocument10 pagesThe Evolving Evidence Base For Child Protection in Chinese SocietiesNORAZLINA BINTI MOHMAD DALI / UPMNo ratings yet
- Online Discussion Forum As A Tool For inDocument8 pagesOnline Discussion Forum As A Tool For inmichael GuduriNo ratings yet
- Characteristics: Talents & TraitsDocument2 pagesCharacteristics: Talents & TraitsTanker117No ratings yet
- Academic HistoryDocument6 pagesAcademic Historyapi-311092584No ratings yet
- Vac STS L100Document20 pagesVac STS L100Safura AliNo ratings yet
- St. Andrews Institute of Technology and Management: Academic Calendar: Btech / Bba / BcaDocument2 pagesSt. Andrews Institute of Technology and Management: Academic Calendar: Btech / Bba / Bcasahil kumarNo ratings yet
- The Mindfulness Acceptance Workbook For Anxiety - Robyn Polsfut Molly HayesDocument25 pagesThe Mindfulness Acceptance Workbook For Anxiety - Robyn Polsfut Molly Hayesapi-308771766100% (1)
- Sujal Sunar CVDocument1 pageSujal Sunar CVkamal joshiNo ratings yet
- Critical EvaluationDocument8 pagesCritical EvaluationMonika SanaaNo ratings yet
- Student Progress Report InstructionsDocument5 pagesStudent Progress Report InstructionsDavidNo ratings yet
- Rules For Robots Get Closer (Pre-Intermediate) PDFDocument5 pagesRules For Robots Get Closer (Pre-Intermediate) PDFCristina OlariuNo ratings yet
- English Q1 M2Document27 pagesEnglish Q1 M2Rosie Florante0% (1)
- Self-Supervised Learning: Generative or ContrastiveDocument20 pagesSelf-Supervised Learning: Generative or ContrastiveIndritNallbaniNo ratings yet
- Melanie Kilgore's Resume - Aug 2012 WITH PorfolioDocument1 pageMelanie Kilgore's Resume - Aug 2012 WITH PorfoliomwkilgoreNo ratings yet
- Event Report: Name of The Event Date(s) Time Venue AgendaDocument5 pagesEvent Report: Name of The Event Date(s) Time Venue Agendamadan mehtaNo ratings yet
- Jurnal Fosil Pollen PDFDocument297 pagesJurnal Fosil Pollen PDFTati FitrianaNo ratings yet
- Conducting BibliographyDocument11 pagesConducting BibliographyThiago Ribeiro100% (1)
- Enerio E. Ebisa..Achievement Test On Philosophies of EducationDocument3 pagesEnerio E. Ebisa..Achievement Test On Philosophies of Educationenerio29No ratings yet
- Natural Resources Lesson PlanDocument3 pagesNatural Resources Lesson PlanJuanita Castro BarreraNo ratings yet
- Dissertation Sur Le Respect Au CollegeDocument8 pagesDissertation Sur Le Respect Au CollegeWriterPaperOmaha100% (1)
- Survival Guide To PHD Students - ZurichDocument194 pagesSurvival Guide To PHD Students - ZurichTapasKumarDash100% (1)
- AEQDocument9 pagesAEQhp937No ratings yet
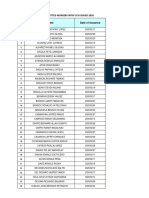
- List of Eps Committed Workers With Ccvi Issued 2020Document4 pagesList of Eps Committed Workers With Ccvi Issued 2020bevlesoyNo ratings yet
- Assessment As Learning PDFDocument11 pagesAssessment As Learning PDFAmineGhobNo ratings yet
- Certificate: Customers For Perfumes and Colognes" Submitted by XXXXX Is A Bonafide Piece of WorkDocument6 pagesCertificate: Customers For Perfumes and Colognes" Submitted by XXXXX Is A Bonafide Piece of WorkramkumarloiNo ratings yet
- IncofyraDocument8 pagesIncofyrachetanNo ratings yet
- Fall 2020 NRP Poster Acp FinalDocument1 pageFall 2020 NRP Poster Acp Finalapi-579593882No ratings yet
- Instructional Planning: School Grade Level Teacher Learning Area Date/Time QuarterDocument2 pagesInstructional Planning: School Grade Level Teacher Learning Area Date/Time QuarterHazel Mae HerreraNo ratings yet
- Modul Year 1 No 2Document8 pagesModul Year 1 No 2Darina Chin AbdullahNo ratings yet