You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Pathophysiology of Disease Flashcards PDFDocument52 pagesPathophysiology of Disease Flashcards PDFFlowerNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pruclinicare Panel ListDocument9 pagesPruclinicare Panel ListMeng Chua60% (5)
- Epidemiology - AMBOSSDocument13 pagesEpidemiology - AMBOSSFlowerNo ratings yet
- CIDP Guideline EJoN 2021Document29 pagesCIDP Guideline EJoN 2021FlowerNo ratings yet
- Mini Project Report FinalDocument24 pagesMini Project Report FinalPrathamesh Parit100% (1)
- Introduction To Biomedical Sciences Individual AssignmentDocument1 pageIntroduction To Biomedical Sciences Individual AssignmentFlowerNo ratings yet
- Latest CbseDocument24 pagesLatest CbseFlowerNo ratings yet
- 1.5 - GI BleedingDocument2 pages1.5 - GI BleedingFlowerNo ratings yet
- 1.3 - Skeletal-Muscle-Relaxants-S3-W9Document2 pages1.3 - Skeletal-Muscle-Relaxants-S3-W9FlowerNo ratings yet
- Developmental Abnormalities of Bone BG Part Without ExplanationsDocument4 pagesDevelopmental Abnormalities of Bone BG Part Without ExplanationsFlowerNo ratings yet
- 2.1 - Advanced DNA TechnologyDocument1 page2.1 - Advanced DNA TechnologyFlowerNo ratings yet
- 2.2 - Drugs-for-Osteoporosis-S3-W9Document2 pages2.2 - Drugs-for-Osteoporosis-S3-W9FlowerNo ratings yet
- FAB TableDocument4 pagesFAB TableFlowerNo ratings yet
- 4 - 8 Sep 10 - The Origin of SpeciesDocument16 pages4 - 8 Sep 10 - The Origin of SpeciesFlowerNo ratings yet
- Pharmacology of HypertensionDocument4 pagesPharmacology of HypertensionFlower100% (1)
- HMS Diabetes - LMNovak MAIN 2022 03.31.2022Document15 pagesHMS Diabetes - LMNovak MAIN 2022 03.31.2022FlowerNo ratings yet
- Welcome To The World of PsychiatricDocument93 pagesWelcome To The World of PsychiatricFlowerNo ratings yet
- Death and Dying - RepairDocument2 pagesDeath and Dying - RepairFlowerNo ratings yet
- 19 Enolates EnaminesDocument59 pages19 Enolates EnaminesFlowerNo ratings yet
- Lecture 11: Random Mating and The Hardy-Weinberg PrincipleDocument6 pagesLecture 11: Random Mating and The Hardy-Weinberg PrincipleFlowerNo ratings yet
- Bio 436 Course SyllabusDocument3 pagesBio 436 Course SyllabusFlowerNo ratings yet
- MutationDocument12 pagesMutationFlowerNo ratings yet
- 4 AnemiaDocument14 pages4 AnemiaFlowerNo ratings yet
- 04Swt PathoDocument89 pages04Swt PathoFlowerNo ratings yet
- 2020 Molecular Biochemistry Handout PDFDocument12 pages2020 Molecular Biochemistry Handout PDFFlowerNo ratings yet
- ReKAP dAY 7Document2 pagesReKAP dAY 7FlowerNo ratings yet
- GlycolysisDocument17 pagesGlycolysisFlowerNo ratings yet
- Metabolism Q and ADocument86 pagesMetabolism Q and AFlowerNo ratings yet
- Four Major Drug TargetsDocument34 pagesFour Major Drug TargetsFlowerNo ratings yet
- U World Day 8Document5 pagesU World Day 8FlowerNo ratings yet
- Metabolic BiochemDocument38 pagesMetabolic BiochemFlowerNo ratings yet
- TA Dr. Julie: TA Dr. Julie: TA Dr. Julie: TA Dr. JulieDocument2 pagesTA Dr. Julie: TA Dr. Julie: TA Dr. Julie: TA Dr. JulieFlowerNo ratings yet
- C&S Financial AnalysisDocument54 pagesC&S Financial AnalysishemantNo ratings yet
- DrSueMorter The Top 3 Mistakes E Book Final 9 18 19Document28 pagesDrSueMorter The Top 3 Mistakes E Book Final 9 18 19Subash Chandar100% (8)
- CFSEI Tech Note X Bracing L001-09Document8 pagesCFSEI Tech Note X Bracing L001-09Jane EyreNo ratings yet
- Chapter 1 - Production and Operations ManagementDocument4 pagesChapter 1 - Production and Operations Managementhello_khayNo ratings yet
- Gen Chem 2Document2 pagesGen Chem 2Trisha Camille MacarioNo ratings yet
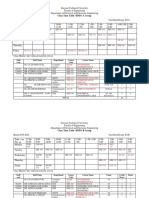
- HND-Class Time Table 1.1Document7 pagesHND-Class Time Table 1.1rajalingamNo ratings yet
- Lab 07 Ballistic PendulumDocument3 pagesLab 07 Ballistic PendulumShahid Iltaf QureshiNo ratings yet
- Humanising Architecture: Case Study ofDocument45 pagesHumanising Architecture: Case Study ofRaghu KrishNo ratings yet
- New - Holland - TM - Electric 199 256Document57 pagesNew - Holland - TM - Electric 199 256Nando100% (1)
- Fluffy Hair - Recherche GoogleDocument1 pageFluffy Hair - Recherche GoogleEliot MaillouxNo ratings yet
- Week 5 - Design Automation - Lecture PresentationDocument39 pagesWeek 5 - Design Automation - Lecture PresentationsrinivaskayalaNo ratings yet
- Waiting For GodotDocument2 pagesWaiting For GodotIoana OlteanuNo ratings yet
- Shell and CoilDocument3 pagesShell and CoilJasperTanNo ratings yet
- Sequanatial Analysis David Siegmund 1985Document285 pagesSequanatial Analysis David Siegmund 1985Jack SmithNo ratings yet
- Car HUD - Windscreen Display For Speed & Compass - Arduino Project HubDocument31 pagesCar HUD - Windscreen Display For Speed & Compass - Arduino Project HubPhops FrealNo ratings yet
- X2R ATOWEB B NRI 003 01 - ATO - Webinar - SlidesDocument67 pagesX2R ATOWEB B NRI 003 01 - ATO - Webinar - SlidesBrik MalekNo ratings yet
- Asera - BKM Id CardDocument35 pagesAsera - BKM Id CardYos JagusNo ratings yet
- Hyperglycemia in Pregnant Ladies and Its Outcome Out in The Opd, Labor Ward, Gynecology and Obstetrics, Lady Atichison Hospital, LahoreDocument7 pagesHyperglycemia in Pregnant Ladies and Its Outcome Out in The Opd, Labor Ward, Gynecology and Obstetrics, Lady Atichison Hospital, LahoreiajpsNo ratings yet
- Entrep Las Second QuarterDocument18 pagesEntrep Las Second QuarterAlodia Carlos PastorizoNo ratings yet
- Gawad Sa Manlilikha NG BayanDocument20 pagesGawad Sa Manlilikha NG Bayanmontefalcothea147No ratings yet
- Wcfs2019 FlyerDocument10 pagesWcfs2019 FlyerZhi Yung TayNo ratings yet
- Places in Town For All Fantasy RPGsDocument15 pagesPlaces in Town For All Fantasy RPGsBob LepNo ratings yet
- Topography - AmravatiDocument32 pagesTopography - AmravatiHi-End SurveysNo ratings yet
- EV ProSound Speaker and Electronics FullCatalog - LR-spreadDocument40 pagesEV ProSound Speaker and Electronics FullCatalog - LR-spreadgreggles69No ratings yet
- TS21.C11.CT01 Consolidated Test-1 On Electronic Configuration and Periodic Properties 13-06-2021 Answer KeyDocument14 pagesTS21.C11.CT01 Consolidated Test-1 On Electronic Configuration and Periodic Properties 13-06-2021 Answer KeyRAVI ANANTHAKRISHNANNo ratings yet
- Drugs Acting On The Nervous SystemDocument123 pagesDrugs Acting On The Nervous SystemIretiola AdeleruNo ratings yet
- PG-300 Portable Gas Analyzer - HORIBADocument2 pagesPG-300 Portable Gas Analyzer - HORIBAKaisar JamilNo ratings yet
- Seam 4 Semi Final ExamDocument2 pagesSeam 4 Semi Final ExamKe Ken EstenzoNo ratings yet