You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Goal and Scope of PsychotherapyDocument4 pagesGoal and Scope of PsychotherapyJasroop Mahal100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Science of Being - 27 Lessons (1-9) - Eugene FersenDocument202 pagesScience of Being - 27 Lessons (1-9) - Eugene FersenOnenessNo ratings yet
- PayPal Verification Guide - AllienwareDocument14 pagesPayPal Verification Guide - Allienware1.o2asNo ratings yet
- Mobile Tower and Mobile Phone Radiation Hazards - Prof Girish Kumar - June 2013Document50 pagesMobile Tower and Mobile Phone Radiation Hazards - Prof Girish Kumar - June 2013Neha Kumar100% (1)
- Ef3e Upper-Inter WL PDFDocument32 pagesEf3e Upper-Inter WL PDFDubravka Kovacevic100% (2)
- Inc. Magazine - 09.2022Document172 pagesInc. Magazine - 09.2022Aman SharmaNo ratings yet
- Complementaria-Sternheimer-Malbin Staining To Detect Decoy Cells in Urine of 213Document6 pagesComplementaria-Sternheimer-Malbin Staining To Detect Decoy Cells in Urine of 213Roberto GutierrezNo ratings yet
- Platelet Transfusion Induces Alloimmunization To D and Non-D Rhesus AntigensDocument6 pagesPlatelet Transfusion Induces Alloimmunization To D and Non-D Rhesus AntigensRoberto GutierrezNo ratings yet
- Current Trends in Platelet Transfusions Practice - The Role of ABO-RhD and Human Leukocyte Antigen IncompatibilityDocument13 pagesCurrent Trends in Platelet Transfusions Practice - The Role of ABO-RhD and Human Leukocyte Antigen IncompatibilityRoberto GutierrezNo ratings yet
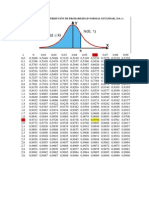
- Áreas Bajo La Distribución de Probabilidad Normal Estándar, N (0, 1)Document1 pageÁreas Bajo La Distribución de Probabilidad Normal Estándar, N (0, 1)Roberto GutierrezNo ratings yet
- Ewc CG 17 6Document942 pagesEwc CG 17 6Milan MarićNo ratings yet
- The PotometerDocument6 pagesThe PotometerRonald Deck Yami100% (1)
- EC - B1P - Language Test 6CDocument6 pagesEC - B1P - Language Test 6CMałgorzata GregorowiczNo ratings yet
- ST ND: Page 1 of 3 BAC Reso No. - S. 2020Document3 pagesST ND: Page 1 of 3 BAC Reso No. - S. 2020Federico DomingoNo ratings yet
- Measure and IntegralDocument5 pagesMeasure and Integralkbains7No ratings yet
- Cobol: School of MAINFRAMESDocument75 pagesCobol: School of MAINFRAMESvendhan123No ratings yet
- Hsep-05 - Communication, Participation & ConsultationDocument6 pagesHsep-05 - Communication, Participation & ConsultationScha AffinNo ratings yet
- SCIDDocument9 pagesSCIDgarimaupadhyay20002No ratings yet
- Oglej Case Study 4300 1Document20 pagesOglej Case Study 4300 1api-533010905No ratings yet
- MEC Activities TimelineDocument13 pagesMEC Activities TimelineFranz Xavier GarciaNo ratings yet
- The Dynamics of Hate Speech and Counter Speech in The Social Media - English 1Document16 pagesThe Dynamics of Hate Speech and Counter Speech in The Social Media - English 1A MNo ratings yet
- Seloka: Jurnal Pendidikan Bahasa Dan Sastra Indonesia: Susilo Rini & WagiranDocument7 pagesSeloka: Jurnal Pendidikan Bahasa Dan Sastra Indonesia: Susilo Rini & Wagiranareni yulitawatiNo ratings yet
- Ricardo Vargas Simplified Pmbok Flow 6ed PROCESSES EN-A4 PDFDocument1 pageRicardo Vargas Simplified Pmbok Flow 6ed PROCESSES EN-A4 PDFFrancisco Alfonso Durán MaldonadoNo ratings yet
- Howo SCR Tenneco. ManualDocument42 pagesHowo SCR Tenneco. Manualulyssescurimao1No ratings yet
- 100 Golden Rules of English Grammar For Error Detection and Sentence ImprovementDocument8 pages100 Golden Rules of English Grammar For Error Detection and Sentence ImprovementHajra bibiNo ratings yet
- CVS Series E 1 6 Inch March 2021 1Document16 pagesCVS Series E 1 6 Inch March 2021 1iqmpslabNo ratings yet
- 7.1.4 Environment For The Operation of ProcessesDocument2 pages7.1.4 Environment For The Operation of ProcessesGVS RaoNo ratings yet
- Css Applied Mathematics2 2009 PDFDocument2 pagesCss Applied Mathematics2 2009 PDFSaleemAhmadMalikNo ratings yet
- Assignment Operational BudgetDocument4 pagesAssignment Operational BudgetBona HirkoNo ratings yet
- A Literary Voyage Into The Unconscious: A Philosophical Approach To The Psychological Novel in Woolf's Mrs. Dalloway (1925)Document10 pagesA Literary Voyage Into The Unconscious: A Philosophical Approach To The Psychological Novel in Woolf's Mrs. Dalloway (1925)Muhammad IbrahimNo ratings yet
- Impact of COVID-19 On Student LifeDocument10 pagesImpact of COVID-19 On Student LifeZunii MalikNo ratings yet
- Migrant Nurses Ausi Integrative ReviewDocument7 pagesMigrant Nurses Ausi Integrative ReviewBony Yunaria TanuNo ratings yet
- WWW - Universityquestions.in: Question BankDocument11 pagesWWW - Universityquestions.in: Question BankgokulchandruNo ratings yet
- Google Maps Places Scraper 19 Jul 2022Document16 pagesGoogle Maps Places Scraper 19 Jul 2022K. SanjuNo ratings yet