You might also like
- MD1187 Recruit Vaccination Form E-Version 13Document2 pagesMD1187 Recruit Vaccination Form E-Version 13Isara Nimcharoen100% (1)
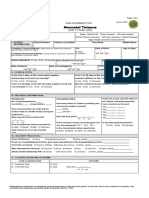
- Dd/Mm/Yyyy Dd/Mm/Yyyy Dd/Mm/YyyyDocument6 pagesDd/Mm/Yyyy Dd/Mm/Yyyy Dd/Mm/YyyyJohn50% (2)
- Human Reproductive BiologyDocument22 pagesHuman Reproductive BiologyAman Santosh TiwariNo ratings yet
- Case Study 1.1. The Nurse Who Told A Lie: Did The Nurse Do The Right Thing? Was The Doctor's Advice Good Advice?Document12 pagesCase Study 1.1. The Nurse Who Told A Lie: Did The Nurse Do The Right Thing? Was The Doctor's Advice Good Advice?Payal NaiduNo ratings yet
- Form 2D Health Plan Implementation Pregnancy Prenatal Care-1Document2 pagesForm 2D Health Plan Implementation Pregnancy Prenatal Care-1Julienne HernandezNo ratings yet
- FORM 2E: Health Plan Implementation For: Maternal Health: Post-Partum CareDocument2 pagesFORM 2E: Health Plan Implementation For: Maternal Health: Post-Partum CarePaul Mark PilarNo ratings yet
- FORM 2C: Health Plan Implementation For CHILD HEALTH (Ages 12 Mos-5 Years)Document2 pagesFORM 2C: Health Plan Implementation For CHILD HEALTH (Ages 12 Mos-5 Years)Paul Mark PilarNo ratings yet
- FORM 2B: Health Plan Implementation For INFANT HEALTH: (Ages 29 Days-Less Than 12 Months)Document2 pagesFORM 2B: Health Plan Implementation For INFANT HEALTH: (Ages 29 Days-Less Than 12 Months)Paul Mark PilarNo ratings yet
- Complete Care Plan Form 508Document5 pagesComplete Care Plan Form 508RSUD SangkulirangNo ratings yet
- Message For F3 and F4: (Last Name, First Name, Mother's Maiden Name)Document2 pagesMessage For F3 and F4: (Last Name, First Name, Mother's Maiden Name)Paul Mark PilarNo ratings yet
- Birth PlanDocument2 pagesBirth PlanAnn Camille RosalesNo ratings yet
- Complete Care Plan Form 508Document5 pagesComplete Care Plan Form 508jobin stanleyNo ratings yet
- IDEAL Discharge Planning Overview, Process, and ChecklistDocument8 pagesIDEAL Discharge Planning Overview, Process, and Checklistrisa agustinaNo ratings yet
- FRM GPPF en 0516Document2 pagesFRM GPPF en 0516Adel NewtonNo ratings yet
- Strat4 Tool 1 IDEAL CHKLST 508Document9 pagesStrat4 Tool 1 IDEAL CHKLST 508Ibsa AbdoNo ratings yet
- Cif NTDocument2 pagesCif NTIvy marie BonNo ratings yet
- Treatment Guarantee Form: Patient DetailsDocument2 pagesTreatment Guarantee Form: Patient DetailsvlcktorNo ratings yet
- Nursing Plan of Care - FinalDocument2 pagesNursing Plan of Care - Finalapi-449184986No ratings yet
- Maternal Care and ServicesDocument35 pagesMaternal Care and ServicesAaron ConstantinoNo ratings yet
- Case Study1 - Calculating Coverage IndicatorsDocument4 pagesCase Study1 - Calculating Coverage IndicatorstegenatalayNo ratings yet
- CDC - Gov/coronavirus: CAPT Elissa Meites, MD, MPHDocument25 pagesCDC - Gov/coronavirus: CAPT Elissa Meites, MD, MPHahmed gamalNo ratings yet
- Content and Complexity of Consultations in A Provider To P - 2022 - General HospDocument2 pagesContent and Complexity of Consultations in A Provider To P - 2022 - General Hospjingwen2002No ratings yet
- DDB Crypto Event 2014 508Document26 pagesDDB Crypto Event 2014 508skdfkjlNo ratings yet
- Health Immunization Clearance Form: Section A: ImmunizationsDocument3 pagesHealth Immunization Clearance Form: Section A: ImmunizationsFaith SetikNo ratings yet
- Consent Form - Pfizer-Biontech Covid-19 VaccineDocument2 pagesConsent Form - Pfizer-Biontech Covid-19 VaccineRommel Bucasas GarciaNo ratings yet
- COVID-19 Vaccine Consent FormDocument5 pagesCOVID-19 Vaccine Consent FormSiamakNo ratings yet
- De2501fc 2Document4 pagesDe2501fc 2PayPal PlcNo ratings yet
- Company Health Insurance Application: Important InformationDocument8 pagesCompany Health Insurance Application: Important InformationMayar RagabNo ratings yet
- Sa426 1809en FDocument12 pagesSa426 1809en Fammar naeemNo ratings yet
- Sample Scale Ranking en FNCPDocument7 pagesSample Scale Ranking en FNCPABDULRAHMAN MISHARI AL-THABITNo ratings yet
- Tracker-Pregnant Women - Adolescents - HEI - Oct 2023Document82 pagesTracker-Pregnant Women - Adolescents - HEI - Oct 2023Migori ArtNo ratings yet
- End of Life Palliative Care Plan For Patients Living in The Community Final Version April 2021 1619003048Document11 pagesEnd of Life Palliative Care Plan For Patients Living in The Community Final Version April 2021 1619003048Only MrcpNo ratings yet
- Carer Allowance - Medical Report: For A Child Under 16 YearsDocument12 pagesCarer Allowance - Medical Report: For A Child Under 16 YearsarishmaawadhNo ratings yet
- CDC Des Update PDFDocument119 pagesCDC Des Update PDFJayanth Bruno SelvarajNo ratings yet
- Family Planning Program: Orientation of NdpsDocument64 pagesFamily Planning Program: Orientation of NdpsMichael Angelo BerdugoNo ratings yet
- Certification of Your Family Member's Serious Health Condition Form - July - 2023Document7 pagesCertification of Your Family Member's Serious Health Condition Form - July - 2023Athenagoras SaldivarNo ratings yet
- Medical Statement New1Document2 pagesMedical Statement New1api-260949827No ratings yet
- CONSENT FORM - COVID-19 VaccineDocument5 pagesCONSENT FORM - COVID-19 Vaccinebersabeh abayNo ratings yet
- Cooper 2020 Emergency Department Grief SupportDocument7 pagesCooper 2020 Emergency Department Grief SupportJuan Andrés Guillermo AnasichaNo ratings yet
- Rajkumar Jangra - N-KOM Health Self Declaration Form Rev 08Document3 pagesRajkumar Jangra - N-KOM Health Self Declaration Form Rev 08tazus subeqiNo ratings yet
- RCare For You Health Declaration For Child Less Than 5 Yrs Ver1.2 (Medical)Document2 pagesRCare For You Health Declaration For Child Less Than 5 Yrs Ver1.2 (Medical)Mexico EnglishNo ratings yet
- Nursing Plan of Care - FinalksDocument6 pagesNursing Plan of Care - Finalksapi-583614158No ratings yet
- PNC - A3-1Document5 pagesPNC - A3-1dabashgetNo ratings yet
- Employer'S Health Insurance Information: State of Utah Department of HealthDocument2 pagesEmployer'S Health Insurance Information: State of Utah Department of HealthJon SmithNo ratings yet
- Employee Health Evaluation & Enrollment Form: Corporate Solutions IncorporatedDocument2 pagesEmployee Health Evaluation & Enrollment Form: Corporate Solutions IncorporatedMitchell BigleyNo ratings yet
- 8.5.20 Gulf COVID-19 UpdateDocument7 pages8.5.20 Gulf COVID-19 Updatemanager2738No ratings yet
- CP 100 PrelimDocument38 pagesCP 100 PrelimDiana FernandezNo ratings yet
- 08.05.20 Covid19 UpdateDocument6 pages08.05.20 Covid19 Updatemanager2738No ratings yet
- Sample Survey - HMO Study - 20HMO - 20studyDocument19 pagesSample Survey - HMO Study - 20HMO - 20studyHebatallah FahmyNo ratings yet
- Welcome Package Adult 2019Document25 pagesWelcome Package Adult 2019David BriggsNo ratings yet
- Flexifed 1 Elect Individual Brochure 2020Document22 pagesFlexifed 1 Elect Individual Brochure 2020BrendanNo ratings yet
- Statement of ChoicesDocument8 pagesStatement of Choicesapi-375641313No ratings yet
- Blencowe2012 National, Regional, and Worldwide Estimates of Preterm Birth Rates in The Year 2010 With Time Trends Since 1990 For Selected Countries, A Systematic Analysis and Implications.Document11 pagesBlencowe2012 National, Regional, and Worldwide Estimates of Preterm Birth Rates in The Year 2010 With Time Trends Since 1990 For Selected Countries, A Systematic Analysis and Implications.diah_budiarti_1No ratings yet
- Senior High School DepartmentDocument46 pagesSenior High School DepartmentErika RodriguezNo ratings yet
- COVID 19 Consent FormDocument2 pagesCOVID 19 Consent FormfvdssfdNo ratings yet
- ReynoldsClinicalSkills CompleteHistoryChecklistDocument5 pagesReynoldsClinicalSkills CompleteHistoryChecklistCRUZ Jill EraNo ratings yet
- Team Lavender Supports Healthcare Workers: "Our Spiritual, Emotional and Mental Health Matters "Document9 pagesTeam Lavender Supports Healthcare Workers: "Our Spiritual, Emotional and Mental Health Matters "Nariman Abed Alganey AkariNo ratings yet
- Allied Therapeutic and Psychology Extender Benefit Application Form 2022Document5 pagesAllied Therapeutic and Psychology Extender Benefit Application Form 2022Kim SnapperNo ratings yet
- NCP GrievingDocument3 pagesNCP GrievingAecee Jose-Macayan100% (4)
- Med School 101 for Patients: A Patient’S Guide to Creating an Exceptional Doctor VisitFrom EverandMed School 101 for Patients: A Patient’S Guide to Creating an Exceptional Doctor VisitNo ratings yet
- Surgical Drains. What The Resident Needs To KnowDocument8 pagesSurgical Drains. What The Resident Needs To Knowginoahnna33No ratings yet
- Prolonging Life or Ridding Illness Without MedicineDocument194 pagesProlonging Life or Ridding Illness Without Medicinecleareye100% (3)
- Artikel Bahasa InggrisDocument1 pageArtikel Bahasa InggrisAna Afifah100% (4)
- PDFDocument9 pagesPDFNikki802No ratings yet
- Fluquadri Vaccine UsageDocument2 pagesFluquadri Vaccine UsageAbhishek Upadhyay100% (1)
- BCI Background Check Reason CodesDocument5 pagesBCI Background Check Reason CodesMike DeWineNo ratings yet
- Self-Directed Learning (Nur 146 - Clinical Area)Document2 pagesSelf-Directed Learning (Nur 146 - Clinical Area)Dyan Bianca Suaso LastimosaNo ratings yet
- Cardiac Output Monitoring - Invasive and Noninvasive - Virendra 2022Document8 pagesCardiac Output Monitoring - Invasive and Noninvasive - Virendra 2022Luis CortezNo ratings yet
- Edinburgh Depression Scale Translated Government of Western Australia Department of HealthDocument271 pagesEdinburgh Depression Scale Translated Government of Western Australia Department of HealthErlangga Perwira Negara100% (1)
- MedicineDocument2 pagesMedicineNurse_ZibaNo ratings yet
- Certificate of Experience: D.V.Srikalpana KannanDocument2 pagesCertificate of Experience: D.V.Srikalpana KannanbalasudhakarNo ratings yet
- Bhatti NotesDocument100 pagesBhatti NotesSergio Chang100% (2)
- Annex C List of Tasks and ActivitiesDocument4 pagesAnnex C List of Tasks and ActivitieskatrinamariembunagNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakagisnamarthaNo ratings yet
- Home Massage-Transforming Family Life Through The Healing Power of TouchDocument209 pagesHome Massage-Transforming Family Life Through The Healing Power of TouchYudhi FaisalNo ratings yet
- Preoperative Evaluation of The Aesthetic PatientDocument36 pagesPreoperative Evaluation of The Aesthetic PatientateeshboroleNo ratings yet
- Opiate Abuse PaperDocument7 pagesOpiate Abuse Paperapi-272576949No ratings yet
- Circulation Sheet 1K1Document2 pagesCirculation Sheet 1K1Ruth LumibaoNo ratings yet
- SAILMediclaim Scheme Guidline 2011Document4 pagesSAILMediclaim Scheme Guidline 2011Bibhu Ranjan PatraNo ratings yet
- Pilot Testing of Triage Coding System in Home-Based Palliative Care Using Edmonton Symptom Assessment ScaleDocument6 pagesPilot Testing of Triage Coding System in Home-Based Palliative Care Using Edmonton Symptom Assessment ScaleMehak KhannaNo ratings yet
- Myasthenia GravisDocument11 pagesMyasthenia Gravishironbose50% (2)
- SynopsysDocument17 pagesSynopsyshellogrkNo ratings yet
- PeKa B40 Personal Data Consent Form - EN - 201901Document1 pagePeKa B40 Personal Data Consent Form - EN - 201901Ezanii ShaharuddinNo ratings yet
- Khiveh 2017Document8 pagesKhiveh 2017Siti lestarinurhamidahNo ratings yet
- Aqsha 2 16-12-2018Document7 pagesAqsha 2 16-12-2018Jody Fajar HibatullahNo ratings yet
- Outcome and Prognosis GDDDocument20 pagesOutcome and Prognosis GDDIfah Inayah D'zatrichaNo ratings yet
- Maternal in ChildDocument15 pagesMaternal in ChildRenalyn VillasencioNo ratings yet
- NZMFM SGA Guideline FinallllDocument29 pagesNZMFM SGA Guideline FinallllShane PangilinanNo ratings yet