You might also like
- Sensory Profile and Plan For SupportingDocument22 pagesSensory Profile and Plan For SupportingAyra Magpili100% (1)
- Tactile Defensiveness &autismDocument10 pagesTactile Defensiveness &autismSushena SharmaNo ratings yet
- Suggestions for Modifying the Home and School Environment: A Handbook for ParentsFrom EverandSuggestions for Modifying the Home and School Environment: A Handbook for ParentsNo ratings yet
- Supporting Therapy in The Classroom Strategies For OccupationalDocument70 pagesSupporting Therapy in The Classroom Strategies For Occupationalapi-451269263No ratings yet
- The Sensory Side Heavy Work Tip SheetDocument2 pagesThe Sensory Side Heavy Work Tip SheetPriyanka MishraNo ratings yet
- Examples of Occupational Therapy Goals For Sensory IntegrationDocument6 pagesExamples of Occupational Therapy Goals For Sensory IntegrationNaza AbdullahNo ratings yet
- Sensory Profile 2 (SP2) : Age Range: Time To AdministerDocument3 pagesSensory Profile 2 (SP2) : Age Range: Time To Administer宗轶烜No ratings yet
- Dyssemia Rating ScaleDocument8 pagesDyssemia Rating ScaleHazardous7No ratings yet
- General Self-Efficacy Scale (GSE)Document2 pagesGeneral Self-Efficacy Scale (GSE)Angelus MoreNo ratings yet
- The Wessex Head Injury MatrixDocument11 pagesThe Wessex Head Injury MatrixLiz GonzálezNo ratings yet
- PEDS DM Developmental Milestone SurveryDocument1 pagePEDS DM Developmental Milestone SurveryNikolayNo ratings yet
- Sensory Profile: Submitted By-Amandeep Kaur M.O.T-Neuro, Sem 3 ENROLLMENT NO - A138141620004 Guided by - Ruby Ma'AmDocument42 pagesSensory Profile: Submitted By-Amandeep Kaur M.O.T-Neuro, Sem 3 ENROLLMENT NO - A138141620004 Guided by - Ruby Ma'Amamandeep kaur100% (1)
- GARS - Report FormatDocument1 pageGARS - Report FormatNazema_SagiNo ratings yet
- Sensory Play ToolkitDocument24 pagesSensory Play ToolkitShah MansiNo ratings yet
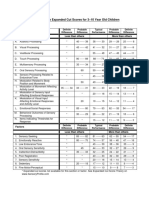
- Sensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenDocument1 pageSensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenAyra MagpiliNo ratings yet
- Sensory Activities: ProprioceptionDocument3 pagesSensory Activities: ProprioceptionPriyanka MishraNo ratings yet
- Ota Watertown Si Clinical Assessment WorksheetDocument4 pagesOta Watertown Si Clinical Assessment WorksheetPaulinaNo ratings yet
- Occupational Therapy Ia Sample ReportsDocument11 pagesOccupational Therapy Ia Sample Reportssneha duttaNo ratings yet
- Tips For Sensory-ProcessingDocument6 pagesTips For Sensory-ProcessingDamayanti Thapa100% (1)
- Making Sense Sensory Processing Disorder103114Document61 pagesMaking Sense Sensory Processing Disorder103114Branislava Jaranovic Vujic100% (5)
- Short Sensory ProfileDocument2 pagesShort Sensory ProfileFatima Zahra PatelNo ratings yet
- BRIEF2 Fact SheetDocument2 pagesBRIEF2 Fact Sheethamzabtoush02No ratings yet
- Sensory Profile 2 Webinar SlidesDocument33 pagesSensory Profile 2 Webinar SlidesCristiane Luiza100% (1)
- Functional AssesmentDocument9 pagesFunctional AssesmentMonica AdamNo ratings yet
- Do You Know Me Flyer-Teacher VersionDocument1 pageDo You Know Me Flyer-Teacher VersionMaria Guy Del DucaNo ratings yet
- Occupational Therapy Sensory Integration Protocol For Early InterDocument56 pagesOccupational Therapy Sensory Integration Protocol For Early Intermanali vyasNo ratings yet
- Sensory Environment AssessmentDocument2 pagesSensory Environment AssessmentDamayanti ThapaNo ratings yet
- The Movment ABC Template For Evaluations AB-2 7-10 YearsDocument2 pagesThe Movment ABC Template For Evaluations AB-2 7-10 YearsFerris100% (1)
- Bayley-III Developmental DomainsDocument4 pagesBayley-III Developmental DomainsYuri medrano100% (1)
- Critically Appraised Paper For SOS FeedingDocument6 pagesCritically Appraised Paper For SOS FeedingJohn DoeNo ratings yet
- The Effect of A Two-Week Sensory Diet On Fussy Infants With Regulatory SensDocument8 pagesThe Effect of A Two-Week Sensory Diet On Fussy Infants With Regulatory Sensapi-238703581No ratings yet
- Sensory Processing Booklet For ParentsDocument5 pagesSensory Processing Booklet For Parentsamrut muzumdar100% (1)
- Sensory History QuestionnaireDocument6 pagesSensory History Questionnaireİpek OMUR100% (1)
- Sensory Integration Inventory ItemiDocument4 pagesSensory Integration Inventory Itemidragomir_emilia92No ratings yet
- IL Early Dev Chart WebDocument4 pagesIL Early Dev Chart WebMuhammad Muzammal HussainNo ratings yet
- SPM Quick Tips Handout pg1 16 PDFDocument16 pagesSPM Quick Tips Handout pg1 16 PDFmalviquemeraNo ratings yet
- Activity Monitoring WorksheetDocument2 pagesActivity Monitoring WorksheetRoberto SzenczukNo ratings yet
- HCA YBOCS EditableDocument9 pagesHCA YBOCS EditableSofiaNo ratings yet
- CARSDocument18 pagesCARSzarish.shireenNo ratings yet
- Early Stimulation and Development ActivitiesDocument63 pagesEarly Stimulation and Development ActivitiesRucsandra AvirvareiNo ratings yet
- Social Skills Checklist 9-07-1Document13 pagesSocial Skills Checklist 9-07-1frozenovenNo ratings yet
- Movement ABC 2 Frequently Asked QuestionsDocument8 pagesMovement ABC 2 Frequently Asked QuestionsCat Graverobber Iskariot0% (1)
- Camouflaging in Autism - A Systematic Review - Accepted ManuscriptDocument82 pagesCamouflaging in Autism - A Systematic Review - Accepted ManuscriptGemma Jones100% (1)
- Chapter 8Document30 pagesChapter 8Karla CarazoNo ratings yet
- DyspraxiaDocument10 pagesDyspraxiaSteben MeuerteNo ratings yet
- FAST - Editable (SMM)Document1 pageFAST - Editable (SMM)Stacey MaxwellNo ratings yet
- About Case Studies of ADHD in Childre1Document6 pagesAbout Case Studies of ADHD in Childre1PearlCladelLapidezNo ratings yet
- Space Management: 0 To 6 Months 6 To 12 Months 12 To 18 MonthsDocument4 pagesSpace Management: 0 To 6 Months 6 To 12 Months 12 To 18 MonthsDaNelle McPhaddenNo ratings yet
- Reinforcer InventoryDocument3 pagesReinforcer Inventoryteamirene13100% (4)
- The Bayley Scales of InfantDocument10 pagesThe Bayley Scales of InfantJESUS MARTIN VILLA CARRASCONo ratings yet
- Sensory AssessmentDocument3 pagesSensory Assessmentapi-377724141No ratings yet
- Supporting Children To Participate Successfully in Everyday Life Using Sensory Processing KnowledgeDocument19 pagesSupporting Children To Participate Successfully in Everyday Life Using Sensory Processing Knowledgeapi-26018051100% (1)
- Sensory Inputs NeonatesDocument13 pagesSensory Inputs NeonatesValedaboveNo ratings yet
- Functional Behavior Assessment FormDocument11 pagesFunctional Behavior Assessment FormAlexandruIulianDorneanu100% (1)
- Salhi Beery Vmi Write UpDocument4 pagesSalhi Beery Vmi Write Upapi-547482419No ratings yet
- Ampsmanual Chapters1-4Document52 pagesAmpsmanual Chapters1-4Aymen DabboussiNo ratings yet
- SENSORY INTEGRATION For ASDDocument35 pagesSENSORY INTEGRATION For ASDcitra city100% (1)
- Home Situations QuestionnaireDocument2 pagesHome Situations QuestionnaireMarina SwansonNo ratings yet
- Introduction To Epidemiology: The Basic Science of Public HealthDocument34 pagesIntroduction To Epidemiology: The Basic Science of Public Healthapi-19641337100% (1)
- Effective Leadership Towards The Star Rating Evaluation of Malaysian Seni Gayung Fatani Malaysia Organization PSGFMDocument10 pagesEffective Leadership Towards The Star Rating Evaluation of Malaysian Seni Gayung Fatani Malaysia Organization PSGFMabishekj274No ratings yet
- High PlateletsDocument9 pagesHigh PlateletsHemal VyasNo ratings yet
- The Varsity 39Document254 pagesThe Varsity 39cosmin_bloju8997No ratings yet
- Affidavit - Rural Cess - ManjulaDocument9 pagesAffidavit - Rural Cess - Manjulagebrsf setgwgvNo ratings yet
- SM Project 1Document75 pagesSM Project 1reena Mahadik100% (1)
- Phytophthora InfestansDocument10 pagesPhytophthora Infestansvas2000No ratings yet
- Behaviorism in Daily LifeDocument8 pagesBehaviorism in Daily LifeMichelleTongNo ratings yet
- PDP2 Heart Healthy LP TDocument24 pagesPDP2 Heart Healthy LP TTisi JhaNo ratings yet
- ELDER European Report On Intergenerational LearningDocument74 pagesELDER European Report On Intergenerational LearningAdelina AndreeaNo ratings yet
- Bias, Confounding and Fallacies in EpidemiologyDocument68 pagesBias, Confounding and Fallacies in EpidemiologyShakir KhanNo ratings yet
- Cardiac Science AED G3 Pro - Service ManualDocument78 pagesCardiac Science AED G3 Pro - Service Manualmisu_stefan6141No ratings yet
- Construction of Magic Soak Pit With Locally Available Materials and Economical DesignDocument4 pagesConstruction of Magic Soak Pit With Locally Available Materials and Economical DesignInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Villegas Lucero 1Document8 pagesVillegas Lucero 1api-213921706No ratings yet
- Umbar - Performance Task 7Document3 pagesUmbar - Performance Task 7Bella CiaoNo ratings yet
- Major Neurological Syndromes PDFDocument260 pagesMajor Neurological Syndromes PDFVirlan Vasile Catalin100% (1)
- Attitude of EMPLOYEES in Terms of Compliance of Health and SafetyDocument6 pagesAttitude of EMPLOYEES in Terms of Compliance of Health and SafetyJanice KimNo ratings yet
- STEVENS DRRR Module 6 Opon Christian Joy ADocument7 pagesSTEVENS DRRR Module 6 Opon Christian Joy AAnthony Bryan Cartujano100% (1)
- ID Faktor Faktor Yang Berhubungan Dengan Perilaku Berisiko Remaja Di Kota MakassarDocument11 pagesID Faktor Faktor Yang Berhubungan Dengan Perilaku Berisiko Remaja Di Kota MakassarEva VidiaNo ratings yet
- Bellavista 1000 Technical - SpecificationsDocument4 pagesBellavista 1000 Technical - SpecificationsTri DemarwanNo ratings yet
- Transferring A Dependent Patient From Bed To ChairDocument5 pagesTransferring A Dependent Patient From Bed To Chairapi-26570979No ratings yet
- Open Your Mind To Receive by Catherine Ponder Success Manual Edition 2010 PDFDocument34 pagesOpen Your Mind To Receive by Catherine Ponder Success Manual Edition 2010 PDFjose100% (2)
- WBC DisordersDocument45 pagesWBC DisordersyalahopaNo ratings yet
- Good Knight 420 GPatien ManualDocument30 pagesGood Knight 420 GPatien ManualJose Antonio AlcazarNo ratings yet
- Lecture 1 Introduction To Industrial HygieneDocument40 pagesLecture 1 Introduction To Industrial Hygienesiti zubaidahNo ratings yet
- A Study On Customer Satisfaction Towards: Ankur 2018-19Document10 pagesA Study On Customer Satisfaction Towards: Ankur 2018-19Pubg GamerNo ratings yet
- English Conversation Discussion About AllergiesDocument3 pagesEnglish Conversation Discussion About AllergiesKevin ScottNo ratings yet
- LNG Hazards and SafetyDocument60 pagesLNG Hazards and SafetyFernando GrandaNo ratings yet
- Brasso Metal Polish v1.3 D8340649 PDFDocument10 pagesBrasso Metal Polish v1.3 D8340649 PDFNia PuanNo ratings yet
- Ch5 PDFDocument35 pagesCh5 PDFsandeepNo ratings yet