You might also like
- Handbook of Addictive Disorders: A Practical Guide to Diagnosis and TreatmentFrom EverandHandbook of Addictive Disorders: A Practical Guide to Diagnosis and TreatmentNo ratings yet
- ConfoundingDocument49 pagesConfoundingLusungu S. LupenzaNo ratings yet
- Confounding and Bias in Cohort StudiesDocument32 pagesConfounding and Bias in Cohort StudiesNasir Ahmad100% (1)
- Clinical EpidemiologyDocument26 pagesClinical EpidemiologyDhevi NiaNo ratings yet
- Confounding, Matching, and Related Analysis Issues: Kevin Schwartzman MD Lecture 8a June 22, 2005Document51 pagesConfounding, Matching, and Related Analysis Issues: Kevin Schwartzman MD Lecture 8a June 22, 2005Santi PadmasariNo ratings yet
- Lecture 10 - Generalizability EMM - Keyes-1Document66 pagesLecture 10 - Generalizability EMM - Keyes-1Ziqian HENo ratings yet
- UntitledDocument5 pagesUntitledYousaku OzakiNo ratings yet
- Case Control StudyDocument19 pagesCase Control Studysara fekriNo ratings yet
- Sec A Confounding and VariabilityDocument15 pagesSec A Confounding and VariabilityLabiba TasnimNo ratings yet
- Evaluating The Role of ConfoundingDocument38 pagesEvaluating The Role of ConfoundingSrinivas KasiNo ratings yet
- Analysis of Cause Effect RelationshipDocument50 pagesAnalysis of Cause Effect RelationshipRida AwwalNo ratings yet
- Materi - Confounders in Internal Validity - GM IPBDocument21 pagesMateri - Confounders in Internal Validity - GM IPBsalehahnhNo ratings yet
- 4) AfeworkDocument193 pages4) AfeworkFoyye Merga GudetaNo ratings yet
- Research Methods 2Document55 pagesResearch Methods 2Dr Ahmed NabilNo ratings yet
- Critical Appraisal of Prognostic StudiesDocument31 pagesCritical Appraisal of Prognostic StudiesInge Nolia Purwita SiwiNo ratings yet
- Modules 5-6Document9 pagesModules 5-6Kevin Yixi RenNo ratings yet
- Logistic Regression and ConfoundingDocument48 pagesLogistic Regression and Confoundingds532No ratings yet
- Session1 Intro Epi 0Document38 pagesSession1 Intro Epi 0Faseeh UllahNo ratings yet
- BIAS. Confounding and Effect ModificationDocument10 pagesBIAS. Confounding and Effect ModificationCSilva16No ratings yet
- Threats To Research Bias and Error Confounding and InteractionDocument8 pagesThreats To Research Bias and Error Confounding and Interactionnajdah_220754970No ratings yet
- Topic 2 - Uses of EpidemiologyDocument51 pagesTopic 2 - Uses of EpidemiologymustafaNo ratings yet
- Bias in ResearchDocument45 pagesBias in ResearchIheakachi IheakachiNo ratings yet
- Theory of CausalityDocument18 pagesTheory of CausalityMazayazka Zahiya ShofiNo ratings yet
- Pengenalan Jenis Penelitian Kesehatan 2014Document22 pagesPengenalan Jenis Penelitian Kesehatan 2014yana marianaNo ratings yet
- Lecture8 NoncomparabilityII 2018Document70 pagesLecture8 NoncomparabilityII 2018Ziqian HENo ratings yet
- Bias & ConfoundingDocument34 pagesBias & ConfoundingdrvikrantkabirpanthiNo ratings yet
- Epidemiology 8: Fundamentals of Statistical & Epidemiological InferenceDocument31 pagesEpidemiology 8: Fundamentals of Statistical & Epidemiological InferenceBaoz PingNo ratings yet
- How To Appraise Harm JournalDocument26 pagesHow To Appraise Harm Journalmirfanjee89No ratings yet
- Confounding TranslateDocument19 pagesConfounding TranslateJonesius Eden ManoppoNo ratings yet
- Observational Studies NCDsDocument58 pagesObservational Studies NCDsAfsana TasnimNo ratings yet
- EPIDIMIOLOGYDocument70 pagesEPIDIMIOLOGYRidwan SulaimanNo ratings yet
- 4 Bias and Causal Associations in Observational Research Grimes2002 PDFDocument5 pages4 Bias and Causal Associations in Observational Research Grimes2002 PDFBenor Amri MustaqimNo ratings yet
- Methods of Comparison: Controlled Experiments and Observational StudiesDocument43 pagesMethods of Comparison: Controlled Experiments and Observational StudiessakiaslamNo ratings yet
- Bias PenelitianDocument27 pagesBias PenelitianAriyati MandiriNo ratings yet
- Causal I DadDocument41 pagesCausal I DadYover Lucero CuevaNo ratings yet
- Analysis of Epidemiologic Studies: Exploring The Role of Errors in MeasurementDocument36 pagesAnalysis of Epidemiologic Studies: Exploring The Role of Errors in Measurementnancynjuguna266No ratings yet
- CEPI5100 - M4 - Course NotesDocument21 pagesCEPI5100 - M4 - Course NotesKarsana ParameswaranNo ratings yet
- Epi Controlling For ConfoundingDocument4 pagesEpi Controlling For ConfoundingcharlesNo ratings yet
- Lecture 8Document18 pagesLecture 8Kanwal KhanNo ratings yet
- Nested Case Control StudyDocument6 pagesNested Case Control StudyFarah FarahNo ratings yet
- Understanding Absolute and Relative RiskDocument7 pagesUnderstanding Absolute and Relative RiskYet AnotherNo ratings yet
- Case ControlDocument45 pagesCase ControlIsmail QamarNo ratings yet
- Potential Errors in Epidemiological StudiesDocument15 pagesPotential Errors in Epidemiological StudiesEric Gyamfi0% (1)
- HomeworkDocument6 pagesHomeworkHumphrey MashetiNo ratings yet
- Confounders, Effect Modifiers and SpuriousDocument4 pagesConfounders, Effect Modifiers and Spuriouswedikaf807No ratings yet
- Eterogeneity 9.1.: 9.1.1. What Do We Mean by Heterogeneity?Document64 pagesEterogeneity 9.1.: 9.1.1. What Do We Mean by Heterogeneity?Anindita Chakraborty100% (1)
- TherappraisalclrDocument5 pagesTherappraisalclrMike CabotageNo ratings yet
- Cause and Effect Relationship - PPTX Latest BinaDocument37 pagesCause and Effect Relationship - PPTX Latest BinaHaalaNo ratings yet
- Avoiding Medical Errors in General PracticeDocument5 pagesAvoiding Medical Errors in General PracticeLaura RossiNo ratings yet
- Stats Notes PartsDocument6 pagesStats Notes PartsPawanNo ratings yet
- Causation and Bias: Prof. Joseph Ntaganira, MD, PHDDocument0 pagesCausation and Bias: Prof. Joseph Ntaganira, MD, PHDJamesNo ratings yet
- PHPS30020 Week1 - 29nov2023 (Effect Measures Estimates of Risk)Document24 pagesPHPS30020 Week1 - 29nov2023 (Effect Measures Estimates of Risk)Katie NolanNo ratings yet
- Validity of Epi Studies 2019Document26 pagesValidity of Epi Studies 2019teklayNo ratings yet
- Is 30 The Magic Number? Issues in Sample Size Estimation: Current TopicDocument5 pagesIs 30 The Magic Number? Issues in Sample Size Estimation: Current TopicJair ArellanoNo ratings yet
- Glossary Concepts - Sensitivity, Specificity & Likelihood RatiosDocument4 pagesGlossary Concepts - Sensitivity, Specificity & Likelihood RatiosJing CruzNo ratings yet
- Wingila Mpamila Worksheet 8Document2 pagesWingila Mpamila Worksheet 8welcome martinNo ratings yet
- A List A Statistical Definition For The CICM Fellowship ExamDocument5 pagesA List A Statistical Definition For The CICM Fellowship ExamSimon WongNo ratings yet
- Chapter 9 Validity in Epidemiologic Studies Booklet - Final 9may2021Document7 pagesChapter 9 Validity in Epidemiologic Studies Booklet - Final 9may2021Genevieve Magpayo NangitNo ratings yet
- Epid 600 Class 8 BiasDocument51 pagesEpid 600 Class 8 BiasRobinNo ratings yet
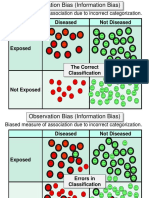
- Diseased Not Diseased: Biased Measure of Association Due To Incorrect CategorizationDocument11 pagesDiseased Not Diseased: Biased Measure of Association Due To Incorrect CategorizationJesus RodriguezNo ratings yet
- Applied Epidemiology: DR Hamid HussainDocument17 pagesApplied Epidemiology: DR Hamid HussainShakir KhanNo ratings yet
- Applied Epidemiology: DR Hamid HussainDocument15 pagesApplied Epidemiology: DR Hamid HussainShakir KhanNo ratings yet
- Applied Epidemiology: DR Hamid HussainDocument10 pagesApplied Epidemiology: DR Hamid HussainShakir KhanNo ratings yet
- 87-Effective Presentations Skills PDFDocument28 pages87-Effective Presentations Skills PDFShakir KhanNo ratings yet
- Define Following Terms ? (I) DisabilityDocument5 pagesDefine Following Terms ? (I) DisabilityShakir KhanNo ratings yet
- Basic Communication SkillsDocument28 pagesBasic Communication SkillsShakir KhanNo ratings yet
- CacaDocument1 pageCacaAgu ArataNo ratings yet
- Research Topic:: Name:Shakir Farid Roll - No: 418 Semester 7Document2 pagesResearch Topic:: Name:Shakir Farid Roll - No: 418 Semester 7Shakir KhanNo ratings yet
- ShakirkhanDocument17 pagesShakirkhanShakir KhanNo ratings yet
- CacaDocument1 pageCacaAgu ArataNo ratings yet
- Redox Biology: Bernard Schmitt, Morgane Vicenzi, Catherine Garrel, Frédéric M. DenisDocument8 pagesRedox Biology: Bernard Schmitt, Morgane Vicenzi, Catherine Garrel, Frédéric M. Denisrocio fernandez san juanNo ratings yet
- Death Due To Fatal Accidental Electrocution A Case ReportDocument4 pagesDeath Due To Fatal Accidental Electrocution A Case ReportDonna WilliamsNo ratings yet
- HOUSE HOLD PERFORMA Final (DR - Syma)Document3 pagesHOUSE HOLD PERFORMA Final (DR - Syma)saraNo ratings yet
- LANCET LOCKDOWN NO MORTALITY BENEFIT A Country Level Analysis Measuring The Impact of Government ActionsDocument8 pagesLANCET LOCKDOWN NO MORTALITY BENEFIT A Country Level Analysis Measuring The Impact of Government ActionsRoger EarlsNo ratings yet
- Management of Lower Extremity TraumaDocument34 pagesManagement of Lower Extremity Trauma정형화No ratings yet
- Lymphatic PDFDocument8 pagesLymphatic PDFJoydee Liza MarcoNo ratings yet
- Congenital SyphilisDocument15 pagesCongenital SyphilisAlejandraSevillaNo ratings yet
- Iron Deficiency Anaemia: LT Col Hamid Iqbal Fcps (Haem) CL Pathologist MH RawalpindiDocument32 pagesIron Deficiency Anaemia: LT Col Hamid Iqbal Fcps (Haem) CL Pathologist MH RawalpindiHamid IqbalNo ratings yet
- Ramsay Hunt SyndromeDocument3 pagesRamsay Hunt SyndromeAnish RajNo ratings yet
- Who PTMDocument234 pagesWho PTMMuniatyNo ratings yet
- Cns Ospe Physiology HandoutDocument24 pagesCns Ospe Physiology HandoutBaby HanmiNo ratings yet
- 5 Science-Backed Secrets For Better SleepDocument26 pages5 Science-Backed Secrets For Better SleepradianteprNo ratings yet
- NeuromatoDocument2 pagesNeuromatoAnonymous hxXpvZdZNo ratings yet
- NCM 109 LectureDocument93 pagesNCM 109 LectureMariah Alexis EncinaNo ratings yet
- 4thQ English Grade 5Document27 pages4thQ English Grade 5diana rose100% (1)
- Occupational Exposure To Fungi and Particles in PoultryDocument176 pagesOccupational Exposure To Fungi and Particles in PoultryFilipe OliveiraNo ratings yet
- Pulmonary Embolism: Amina Adel Al-QaysiDocument37 pagesPulmonary Embolism: Amina Adel Al-QaysiJasleen Kaur100% (2)
- Hemophilia ADocument20 pagesHemophilia Adiaharmayukti100% (1)
- The Nine Supplements Everyone Should TakeDocument4 pagesThe Nine Supplements Everyone Should TakekatiaNo ratings yet
- TE2 - 15 JunDocument186 pagesTE2 - 15 JunPTchongNo ratings yet
- Newsletter BHIS NoidaDocument39 pagesNewsletter BHIS NoidaReshma KhemchandaniNo ratings yet
- National Arogya Fair: Namma BengaluruDocument2 pagesNational Arogya Fair: Namma BengaluruPrajkta AbnaveNo ratings yet
- Scoring and Scaling C1Document3 pagesScoring and Scaling C1Kimberly BongonNo ratings yet
- Pediatric Nursing: Prepared By: ProfDocument4 pagesPediatric Nursing: Prepared By: ProfAllyza Jane SartigaNo ratings yet
- Ultimate Pediatrics Exam Quiz - Trivia! - ProProfs QuizDocument1 pageUltimate Pediatrics Exam Quiz - Trivia! - ProProfs QuizManaye AyalnehNo ratings yet
- (ADA) Package Insert (CE)Document31 pages(ADA) Package Insert (CE)Sinari AlfatNo ratings yet
- 2F Water and ElectrolytesDocument6 pages2F Water and ElectrolytesKaiNo ratings yet
- Lecture Notes On CardiologyDocument31 pagesLecture Notes On CardiologyambiskuysNo ratings yet
- What Is Helen Keller Thesis in The Most Important DayDocument7 pagesWhat Is Helen Keller Thesis in The Most Important Dayaflnoexvofebaf100% (1)
- Q3 - M4 - L1-Judging The Relevance and Worth of Ideas Presented in A Viewing MaterialDocument25 pagesQ3 - M4 - L1-Judging The Relevance and Worth of Ideas Presented in A Viewing MaterialSmiley Jhen Garcia SabinianoNo ratings yet