You might also like
- FMD-F-11-02.14.4 Work Permit Hot Work PermitDocument2 pagesFMD-F-11-02.14.4 Work Permit Hot Work PermitAlvin Bosque50% (2)
- Application Form OSH PractitionerDocument3 pagesApplication Form OSH PractitionerJayvee Baradas Valdez100% (4)
- Module 5 - Emergency Preparedness - BOSH For SO1Document40 pagesModule 5 - Emergency Preparedness - BOSH For SO1NKH Mega GasNo ratings yet
- DOLE - FORM - WAIR - 1 - FOR - February 2023 PDFDocument1 pageDOLE - FORM - WAIR - 1 - FOR - February 2023 PDFKaren Jen100% (3)
- Fire Drill LetterDocument1 pageFire Drill Letterjiero rogel100% (1)
- 003 MARCH 2018 TRAINING SCHEDULE BataanDocument2 pages003 MARCH 2018 TRAINING SCHEDULE BataanAviects Avie Jaro100% (1)
- Turbochef Ngo Service MaualDocument70 pagesTurbochef Ngo Service MaualgboswellNo ratings yet
- BWC-IP3-rev_2011 RegistrationDocument3 pagesBWC-IP3-rev_2011 RegistrationMark Anthony RojoNo ratings yet
- DOLE - Department Order 198-18Document44 pagesDOLE - Department Order 198-18Dwight Agulan100% (1)
- Report of Safety and Health Organization MarilaoDocument1 pageReport of Safety and Health Organization MarilaoМарк Артём Лимот АпаллаNo ratings yet
- OJT Certificate of Completion TemplateDocument1 pageOJT Certificate of Completion TemplateJuliet ChuaNo ratings yet
- Bukidnon State University: Buksu Casisang AnnexDocument2 pagesBukidnon State University: Buksu Casisang Annexjason a. un100% (2)
- Hirac - DoleDocument11 pagesHirac - DoleAngela Salumbides50% (2)
- The Range and Application of Phast and Safeti Explosion Models For Facility Siting Work - 3 December - PresentationDocument60 pagesThe Range and Application of Phast and Safeti Explosion Models For Facility Siting Work - 3 December - PresentationsushantNo ratings yet
- Trauma Stewardship: An Everyday Guide To Caring For Self While Caring For Others - Laura Van Dernoot LipskyDocument5 pagesTrauma Stewardship: An Everyday Guide To Caring For Self While Caring For Others - Laura Van Dernoot Lipskyhyficypo0% (3)
- Edited Sourcebook For Providing TA On PopDev Integration PDFDocument60 pagesEdited Sourcebook For Providing TA On PopDev Integration PDFIbrahim Jade De AsisNo ratings yet
- FTI 2021 Tech Trends Volume AllDocument504 pagesFTI 2021 Tech Trends Volume AlljapamecNo ratings yet
- Government Safety Engineer'S Accident Investigation ReportDocument1 pageGovernment Safety Engineer'S Accident Investigation ReportDon Aries EidosNo ratings yet
- Annual Work Accident/Illness Exposure Data Report: General ManagerDocument1 pageAnnual Work Accident/Illness Exposure Data Report: General ManagerJamil DiligNo ratings yet
- Annual Work Accident/Illness Exposure Data Report: General ManagerDocument1 pageAnnual Work Accident/Illness Exposure Data Report: General ManagerReynaldo PesqueraNo ratings yet
- Osh Program TemplateDocument12 pagesOsh Program TemplateMc alvinth SacletNo ratings yet
- Wair Ip-6 PDFDocument2 pagesWair Ip-6 PDFJMNo ratings yet
- Osh Program EditableDocument12 pagesOsh Program EditableMarivicNo ratings yet
- General Safety Orientation Guideline For The Oil & Gas Industry PDFDocument29 pagesGeneral Safety Orientation Guideline For The Oil & Gas Industry PDFPatricio Romero100% (1)
- Module-5 EmergencyPreparedness BOSHforSO1Document28 pagesModule-5 EmergencyPreparedness BOSHforSO1Joseph CabreraNo ratings yet
- Fire Brigade Organizational ChartDocument1 pageFire Brigade Organizational ChartМарк Артём Лимот Апалла100% (2)
- Monrio Industrial Corporation Turnover FormDocument1 pageMonrio Industrial Corporation Turnover FormJaycee QuinNo ratings yet
- Weekly Safety Report 400KV RAS LEGRAIN ProjectDocument4 pagesWeekly Safety Report 400KV RAS LEGRAIN Projectwinston11No ratings yet
- WAIRDocument1 pageWAIRAlaine SobredoNo ratings yet
- FORM - Dole Employer's Work Accident Illness ReportDocument6 pagesFORM - Dole Employer's Work Accident Illness Reportshirleyaquino675No ratings yet
- Report on Health and Safety Organization at Prudential Customs Brokerage ServicesDocument1 pageReport on Health and Safety Organization at Prudential Customs Brokerage ServicesDaniel Reyes0% (1)
- OSH ProgramDocument14 pagesOSH ProgramCABIGAN, Lady Lee T. 3BNo ratings yet
- Re-Entry Planning in Osh: Name Christian Caldeo Company Date May 31, 2021 Work AreaDocument2 pagesRe-Entry Planning in Osh: Name Christian Caldeo Company Date May 31, 2021 Work AreaVincent PerraNo ratings yet
- PH Bir 0605Document2 pagesPH Bir 0605Anonymous onBMYp9YNo ratings yet
- Eohsms-02-C25 Loa First AiderDocument1 pageEohsms-02-C25 Loa First AiderHassan AbdullahNo ratings yet
- b2230 Boysen Epoxy Primer GrayDocument9 pagesb2230 Boysen Epoxy Primer GrayAlex Joshua Maglasang100% (1)
- Annual Work Accident Illness Exposure Data Report PDFDocument1 pageAnnual Work Accident Illness Exposure Data Report PDFedz100% (1)
- GL-01-EHS-032 Guidelines On Work Environment MeasurementDocument8 pagesGL-01-EHS-032 Guidelines On Work Environment MeasurementClarabelle Mae Dela RosaNo ratings yet
- Bics Ics 211Document6 pagesBics Ics 211DocJogy SalazarNo ratings yet
- BFP Capiz Daily Vehicle CheckDocument2 pagesBFP Capiz Daily Vehicle CheckDondonNo ratings yet
- Loss Control and Safety Management TestDocument6 pagesLoss Control and Safety Management TestELSON MASHAWINo ratings yet
- CSHP COMPREHENSIVE Application FormDocument3 pagesCSHP COMPREHENSIVE Application FormNick Cajan100% (1)
- RSO-Report On Health and Safety OrganizationDocument2 pagesRSO-Report On Health and Safety OrganizationAlaine Sobredo0% (1)
- Template Resigning PCODocument1 pageTemplate Resigning PCOawenskie0% (1)
- Re Entry MARCOS F. FUERTEDocument2 pagesRe Entry MARCOS F. FUERTEvan gerald100% (1)
- Contractors Annual Report 2016Document1 pageContractors Annual Report 2016Anonymous b7mapUNo ratings yet
- REPORT Annual Work Accident DataDocument1 pageREPORT Annual Work Accident Datawindell PatalinghugNo ratings yet
- Application For Safety PractitionerDocument4 pagesApplication For Safety PractitionerMark Rusiana100% (1)
- Hazardous Spill PlanDocument8 pagesHazardous Spill PlanChandan ChamanNo ratings yet
- 2nd Fire Drill 2019Document1 page2nd Fire Drill 2019Jonnel BadillaNo ratings yet
- Occupational Safety and Health Standars: As Amended: Department of Labor and Employment, Manila PhilippinesDocument12 pagesOccupational Safety and Health Standars: As Amended: Department of Labor and Employment, Manila PhilippinesShan AdriasNo ratings yet
- Injury Incident Report FormDocument3 pagesInjury Incident Report FormDave Joseph Conde100% (1)
- MINUTES OF MEETING AprilDocument2 pagesMINUTES OF MEETING AprilAlvin John DionisioNo ratings yet
- Safety Practitioner Accreditation ChecklistDocument2 pagesSafety Practitioner Accreditation Checklistrasales100% (4)
- DTR SecurityDocument1 pageDTR SecurityElizer100% (2)
- 2021.01.12 - Letter - Request For Exit Gate PassDocument1 page2021.01.12 - Letter - Request For Exit Gate PassIsrael FortoNo ratings yet
- 004 Memo - PpeDocument1 page004 Memo - Ppesaf_one22100% (1)
- OSH Law RA 11058 - IRRDocument96 pagesOSH Law RA 11058 - IRRRERREFAIT100% (1)
- TEEM Building Industrial Complex Safety Officer CertificationDocument30 pagesTEEM Building Industrial Complex Safety Officer CertificationJohn Ervin AgenaNo ratings yet
- DO 198 Implementing Rules and Regulations of Republic Act No - 11058 An Act Strengthening Compliance With Occupational Safety and Health Standards and Providing Penalties For Violations Thereof PDFDocument26 pagesDO 198 Implementing Rules and Regulations of Republic Act No - 11058 An Act Strengthening Compliance With Occupational Safety and Health Standards and Providing Penalties For Violations Thereof PDFAlex FelicesNo ratings yet
- Workshop: Computation of Accident's: - Frequency Rate & - Severity RateDocument5 pagesWorkshop: Computation of Accident's: - Frequency Rate & - Severity RateErwin Marc OcampoNo ratings yet
- Sdoc 01 31 SiDocument1 pageSdoc 01 31 SiRafael N. ArellanoNo ratings yet
- Contractor HSE Profile FormDocument2 pagesContractor HSE Profile FormebyjoyNo ratings yet
- Application For Assessment R6Document3 pagesApplication For Assessment R6MMI BatamNo ratings yet
- PRC Benguet Chapter CertificationDocument1 pagePRC Benguet Chapter CertificationPrestone Napiloy Kalang-adNo ratings yet
- Lo To Simple Equip ListDocument1 pageLo To Simple Equip ListPrestone Napiloy Kalang-adNo ratings yet
- PTW 7: Work at Height: Reference NumberDocument2 pagesPTW 7: Work at Height: Reference NumberPrestone Napiloy Kalang-adNo ratings yet
- Cost of Implementing OSH ProgramDocument2 pagesCost of Implementing OSH ProgramPrestone Napiloy Kalang-adNo ratings yet
- Process Flow Diagram of All Waste StreamsDocument1 pageProcess Flow Diagram of All Waste StreamsPrestone Napiloy Kalang-adNo ratings yet
- PO-FG Wilson-Perkins Gen Set (2020-POA-E-141109-1135)Document3 pagesPO-FG Wilson-Perkins Gen Set (2020-POA-E-141109-1135)Prestone Napiloy Kalang-adNo ratings yet
- Ergonomics 2Document19 pagesErgonomics 2EIL WH HAZIRANo ratings yet
- Emergency Preparedness Guide for Workplace Hazards & DisastersDocument28 pagesEmergency Preparedness Guide for Workplace Hazards & DisastersPrestone Napiloy Kalang-adNo ratings yet
- PRC Benguet Chapter CertificationDocument1 pagePRC Benguet Chapter CertificationPrestone Napiloy Kalang-adNo ratings yet
- Machine GuardingDocument47 pagesMachine GuardingPrestone Napiloy Kalang-adNo ratings yet
- Work Accident ReportDocument1 pageWork Accident ReportBryan RuizNo ratings yet
- Safety Awareness and PPE Rev.Document33 pagesSafety Awareness and PPE Rev.Prestone Napiloy Kalang-adNo ratings yet
- Health - Annual Health - Plan - TemplateDocument1 pageHealth - Annual Health - Plan - TemplatePrestone Napiloy Kalang-ad0% (1)
- Annual medical report form insightsDocument5 pagesAnnual medical report form insightsGemarie Adarlo CastilloNo ratings yet
- Hazards, Risks & Controls in OH&S ManagementDocument275 pagesHazards, Risks & Controls in OH&S ManagementPrestone Napiloy Kalang-adNo ratings yet
- OSHA Machine Guarding2Document63 pagesOSHA Machine Guarding2hoan thanhNo ratings yet
- Example Risk Assessment For Food Preparation, Cooking and ServiceDocument6 pagesExample Risk Assessment For Food Preparation, Cooking and ServiceUmair SohailNo ratings yet
- ISO 17025 Lab Risk Assessment: September 2019Document6 pagesISO 17025 Lab Risk Assessment: September 2019Elena Iulia CucoleaNo ratings yet
- Machinery Safety: Machine Guarding For Warehouse and Maintenance WorkersDocument69 pagesMachinery Safety: Machine Guarding For Warehouse and Maintenance WorkersEliana J Yazo CNo ratings yet
- Office Insp TemplateDocument4 pagesOffice Insp TemplatePrestone Napiloy Kalang-adNo ratings yet
- ISO 22000:2018 Foundation CourseDocument64 pagesISO 22000:2018 Foundation CoursePrestone Napiloy Kalang-ad100% (1)
- What Is Management of Change (MOC) ?Document9 pagesWhat Is Management of Change (MOC) ?Prestone Napiloy Kalang-adNo ratings yet
- Food safety checklistDocument2 pagesFood safety checklistMeryem RouissaNo ratings yet
- Vehicle Safety DefensiveDocument18 pagesVehicle Safety DefensivePrestone Napiloy Kalang-adNo ratings yet
- Emergency Drill FormDocument5 pagesEmergency Drill FormPrestone Napiloy Kalang-adNo ratings yet
- Health FIRST AID GUIDEDocument13 pagesHealth FIRST AID GUIDEPrestone Napiloy Kalang-adNo ratings yet
- Hazard Identification Risk Assessment AND Control: Department of Health and Safety ServicesDocument14 pagesHazard Identification Risk Assessment AND Control: Department of Health and Safety ServicesRi OzNo ratings yet
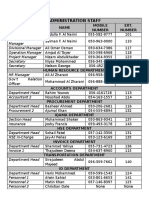
- Administration Staff DirectoryDocument2 pagesAdministration Staff DirectoryPrestone Napiloy Kalang-adNo ratings yet
- Concept Paper (R)Document7 pagesConcept Paper (R)Joseph EneroNo ratings yet
- Innovative Solution For Biomedical Waste ManagementDocument5 pagesInnovative Solution For Biomedical Waste Managementaysh2383No ratings yet
- Pragmatics Kel 2Document10 pagesPragmatics Kel 2i iNo ratings yet
- Circular Building Process Reuse of Insulators From Construction and Demolition Waste To Produce Lime MortarsBuildings PDFDocument25 pagesCircular Building Process Reuse of Insulators From Construction and Demolition Waste To Produce Lime MortarsBuildings PDFGonzalo Fuentes GuimetNo ratings yet
- Vol 5, No 2 November, Pp. 99-111 P-ISSN 2549-4880, E-ISSN 2614-1310 Journal DOI: WebsiteDocument11 pagesVol 5, No 2 November, Pp. 99-111 P-ISSN 2549-4880, E-ISSN 2614-1310 Journal DOI: WebsiteSyarah RamadhaniNo ratings yet
- Design Brief On MEP Systems PDFDocument21 pagesDesign Brief On MEP Systems PDFAdhikari ThushanNo ratings yet
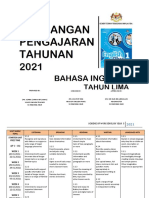
- Sow English Year 5 2021Document14 pagesSow English Year 5 2021AZRINA ZARIFAH BINTI ZAINAL MoeNo ratings yet
- SPEX 201 Lab 1 - Motion Analysis Techniques - STUDENT - 2023Document8 pagesSPEX 201 Lab 1 - Motion Analysis Techniques - STUDENT - 2023tom mallardNo ratings yet
- Phrasal Verbs ListDocument85 pagesPhrasal Verbs ListVirginia E. C.No ratings yet
- SW Lightsaber Guide.2.6.17Document54 pagesSW Lightsaber Guide.2.6.17Jose LimaNo ratings yet
- MB Module 1Document29 pagesMB Module 1sophieNo ratings yet
- Procurement of Land in Indonesia: Challenges and Solutions in the Legal Sociological PerspectiveDocument12 pagesProcurement of Land in Indonesia: Challenges and Solutions in the Legal Sociological PerspectiveFrans OleyNo ratings yet
- QC OF SUPPOSITORIESDocument23 pagesQC OF SUPPOSITORIESHassan kamalNo ratings yet
- PoisonedfoodDocument10 pagesPoisonedfoodMare JNo ratings yet
- CAEN A2518 Rev16Document18 pagesCAEN A2518 Rev16Arnaud RomainNo ratings yet
- CHEMICAL APPROVAL FORMDocument2 pagesCHEMICAL APPROVAL FORMYosep SasadaNo ratings yet
- Labs: Wood Adhesives and Coatings: ScheduleDocument3 pagesLabs: Wood Adhesives and Coatings: ScheduleArnav DasaurNo ratings yet
- Distance Calculation Between 2 Points On EarthDocument3 pagesDistance Calculation Between 2 Points On EarthGirish Madhavan Nambiar100% (2)
- Math (Safal)Document3 pagesMath (Safal)AdowNo ratings yet
- 2018 January Proficiency Session 2 A VersionDocument2 pages2018 January Proficiency Session 2 A VersionUğur GiderNo ratings yet
- 08 - Marian-Avram Vincze, Horatiu-Stefan GrifDocument4 pages08 - Marian-Avram Vincze, Horatiu-Stefan GrifBudiandra Yusuf MahendraNo ratings yet
- GH04.Key Word TransformationDocument6 pagesGH04.Key Word TransformationViệt Hà Nguyễn BùiNo ratings yet
- Assessment of Crude Oil Blends PDFDocument6 pagesAssessment of Crude Oil Blends PDFDanivian HigginsNo ratings yet
- 11 Axis FormationDocument61 pages11 Axis Formationapi-3800038100% (1)
- FundamentalsDocument39 pagesFundamentalsMoses KibikyaboNo ratings yet
- Phonons 1-D Linear Chain of AtomsDocument12 pagesPhonons 1-D Linear Chain of Atomsمؤيد العليNo ratings yet