You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Interface Specification - Dimension - Interface Manual DXDCM 09008b8380544007-1321582685628Document36 pagesInterface Specification - Dimension - Interface Manual DXDCM 09008b8380544007-1321582685628Rupesh Nidhi100% (1)
- Mixing TipsDocument10 pagesMixing TipsyebaimNo ratings yet
- Report Writting SampleDocument302 pagesReport Writting Samplecastro dasNo ratings yet
- A Study of Urbanization in Pune DistrictDocument11 pagesA Study of Urbanization in Pune DistrictDIVYA DAHADNo ratings yet
- Linear TransducerDocument4 pagesLinear TransducerZuky ProzitNo ratings yet
- United States v. Hilario, 218 F.3d 19, 1st Cir. (2000)Document14 pagesUnited States v. Hilario, 218 F.3d 19, 1st Cir. (2000)Scribd Government DocsNo ratings yet
- Oracle EBS Setup Guide (12.2)Document614 pagesOracle EBS Setup Guide (12.2)catlover100% (2)
- Additional Bank GuaranteeDocument3 pagesAdditional Bank Guaranteesammy gaurNo ratings yet
- Steam Jet Air EjectorsDocument3 pagesSteam Jet Air EjectorsSherwin SabandoNo ratings yet
- Rfc35N Nmea Compass: Installation and CalibrationDocument12 pagesRfc35N Nmea Compass: Installation and CalibrationmakenodimaNo ratings yet
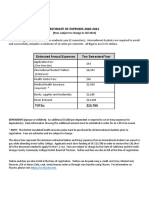
- Estimate of Expenses 2020-2021: (Fees Subject To Change in Fall 2021)Document2 pagesEstimate of Expenses 2020-2021: (Fees Subject To Change in Fall 2021)Walid TaouhidNo ratings yet
- Direct and Indirect Effect of Brand Experience On True Brand Loyalty: Role of InvolvementDocument24 pagesDirect and Indirect Effect of Brand Experience On True Brand Loyalty: Role of InvolvementBilal TanveerNo ratings yet
- Game PDFDocument10 pagesGame PDFKichi UeharaNo ratings yet
- Barangay Disaster Risk Reduction and Management Investment Plan C.Y. 2018-2022Document1 pageBarangay Disaster Risk Reduction and Management Investment Plan C.Y. 2018-2022Cristina MelloriaNo ratings yet
- Qamar Muhammad Noman 00657679 Avt Academy, 1486Document17 pagesQamar Muhammad Noman 00657679 Avt Academy, 1486noumanqamar61No ratings yet
- 2 Feliks (2020) Effective Use of Big DataDocument16 pages2 Feliks (2020) Effective Use of Big DataFeliks SejahteraNo ratings yet
- IBM AIX Enhancements: and ModernizationDocument188 pagesIBM AIX Enhancements: and ModernizationOscar Humberto Torres CarranzaNo ratings yet
- Vdocuments - MX - Zte Bts 8800 Manual PDFDocument2 pagesVdocuments - MX - Zte Bts 8800 Manual PDFEze Alexander IkNo ratings yet
- Go v. Sunbanun and 3. Belgica v. OchcoaDocument4 pagesGo v. Sunbanun and 3. Belgica v. Ochcoajharik23No ratings yet
- Synopsis FormatDocument2 pagesSynopsis FormatIm__NehaThakurNo ratings yet
- Unlawful Detainer AnswerDocument9 pagesUnlawful Detainer AnswerJeneveth SitoyNo ratings yet
- Introduction of The StudyDocument8 pagesIntroduction of The StudyAmey ShingoteNo ratings yet
- 10-1340 enDocument37 pages10-1340 enRodolfo NallisNo ratings yet
- Narrative ReportDocument4 pagesNarrative ReportAnonymous 9sKZvA6P100% (1)
- ReleaseNotes 1 0 2Document2 pagesReleaseNotes 1 0 2Fabio JesusNo ratings yet
- Curriculum Vitae': Anshul PareekDocument3 pagesCurriculum Vitae': Anshul PareekChanchal AgrawalNo ratings yet
- Antivirus CovidDocument12 pagesAntivirus CovidAni RahayuNo ratings yet
- Hms Hmsi 27 316Document135 pagesHms Hmsi 27 316davoodnasehi1No ratings yet
- Contrabending and Reverse Twist As A Basic Biomechanical Force To Correct Deformity in Scoliosis (Revision) Docx PDFDocument11 pagesContrabending and Reverse Twist As A Basic Biomechanical Force To Correct Deformity in Scoliosis (Revision) Docx PDFFahmi AnshoriNo ratings yet
- 11 Kriteria PenerimaanDocument33 pages11 Kriteria PenerimaanMohd Zulhairi Mohd NoorNo ratings yet