You might also like
- Prevalence of Musculoskeletal Pain Among Professional Drivers: A Systematic ReviewDocument17 pagesPrevalence of Musculoskeletal Pain Among Professional Drivers: A Systematic ReviewJENNIFER RIOFRIO ASEICHANo ratings yet
- Transportation Research Interdisciplinary Perspectives: Md. Ebrahim ShaikDocument9 pagesTransportation Research Interdisciplinary Perspectives: Md. Ebrahim ShaikSangeetha NNo ratings yet
- Ergonomic Endeavours To Enhancing Safety and HealtDocument4 pagesErgonomic Endeavours To Enhancing Safety and HealtShree PatelNo ratings yet
- 9 RespiratoryDocument5 pages9 RespiratorySanjay BadigerNo ratings yet
- Ergonomic Assessment of Occupational Health of Transport OperatorsDocument4 pagesErgonomic Assessment of Occupational Health of Transport OperatorsAkbarNo ratings yet
- Accidents 1Document6 pagesAccidents 1oloyede_wole3741No ratings yet
- Yasobantetal - DriverErgonomicsDocument6 pagesYasobantetal - DriverErgonomicsAkbarNo ratings yet
- SI Effect of Activities of Daily Living Status On Resuming Driving After StrokeDocument3 pagesSI Effect of Activities of Daily Living Status On Resuming Driving After StrokeISABEU ANDREA IVANA AYALA VIDALNo ratings yet
- Traffic Accidents Research PaperDocument6 pagesTraffic Accidents Research Paperjrcrefvhf100% (1)
- Ergonomic_risk_assessment_of_working_postures_of_nDocument21 pagesErgonomic_risk_assessment_of_working_postures_of_nberliancantikberlianNo ratings yet
- Work-Related Musculoskeletal Disorders in Iranian Dentists - A Systematic Review and Meta-AnalysisDocument9 pagesWork-Related Musculoskeletal Disorders in Iranian Dentists - A Systematic Review and Meta-AnalysisAbelNo ratings yet
- Ajassp 2010 1087 1092-2Document6 pagesAjassp 2010 1087 1092-2JHON FABER FORERO BARCONo ratings yet
- Driver Performance Evaluation ConsideratDocument10 pagesDriver Performance Evaluation Consideratprofeta1955No ratings yet
- Ergonomics For Electronics Manufacturing: January 2006Document7 pagesErgonomics For Electronics Manufacturing: January 2006andrei CalloNo ratings yet
- Manual Material Handling Assessment and Repetitive Tasks With Two Methods MAC and ART in A Subsidiary of A Manufacturer of Cleaning Products A R T I C L E InfoDocument9 pagesManual Material Handling Assessment and Repetitive Tasks With Two Methods MAC and ART in A Subsidiary of A Manufacturer of Cleaning Products A R T I C L E InfoNORERNY SHUHADA BINTI HAMDANNo ratings yet
- Rob Band Mansfield ArticleDocument30 pagesRob Band Mansfield ArticleJhet CoritanaNo ratings yet
- Occupational Health and Safety Issues of Traffic EnforcersDocument16 pagesOccupational Health and Safety Issues of Traffic EnforcersRhobin Mhark GabitoNo ratings yet
- Exploring Monitoring Systems Data For Driver Distraction and Drowsiness ResearchDocument14 pagesExploring Monitoring Systems Data For Driver Distraction and Drowsiness Researchotik brebesNo ratings yet
- Musculoskeletal Work-Related Disorders and Ergonomic Hazards Among Bank - Employees in State of KuwaitDocument8 pagesMusculoskeletal Work-Related Disorders and Ergonomic Hazards Among Bank - Employees in State of KuwaitInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- project group4Document11 pagesproject group41254107369No ratings yet
- The Prevalence and Risk Factors of Work Related Musculoskeletal Disorders Among Electronics Manufacturing Workers: A Cross-Sectional Analytical Study in ChinaDocument11 pagesThe Prevalence and Risk Factors of Work Related Musculoskeletal Disorders Among Electronics Manufacturing Workers: A Cross-Sectional Analytical Study in ChinaMohamad Ashraf Mohd AminudinNo ratings yet
- Ergonomics Analysis Tools Used in IndustryDocument10 pagesErgonomics Analysis Tools Used in IndustryMyle26No ratings yet
- Nassiopoulosetal WRC Sideimpact 2010Document9 pagesNassiopoulosetal WRC Sideimpact 2010Zhe ChenNo ratings yet
- Ijm 11 04 059Document8 pagesIjm 11 04 059IAEME PublicationNo ratings yet
- The Prevalence of Work-Related Musculoskeletal Disorders in Long-Distance Bus DriversDocument4 pagesThe Prevalence of Work-Related Musculoskeletal Disorders in Long-Distance Bus DriversSatria DananjayaNo ratings yet
- Ergonomics CallcenterworkersDocument9 pagesErgonomics CallcenterworkersAkbarNo ratings yet
- Risk Analysis of Gari FryingDocument13 pagesRisk Analysis of Gari FryingSamuelShinaAyodeleNo ratings yet
- Prevalence of Work Related Musculoskeletal Disorders and Risk Factors Amongst Nurses of Buea and Tiko Health Districts, South West Region, CameroonDocument8 pagesPrevalence of Work Related Musculoskeletal Disorders and Risk Factors Amongst Nurses of Buea and Tiko Health Districts, South West Region, CameroonEditor IJTSRDNo ratings yet
- Improving Ergonomic Conditions at Hospitality InduDocument11 pagesImproving Ergonomic Conditions at Hospitality Indulheilahernandez028No ratings yet
- Mecanica AutomotrizDocument10 pagesMecanica AutomotrizPatricia Zaragoza FloresNo ratings yet
- SPE-177117-MS Learning by Impact Driving Training: A Case Study From EcuadorDocument5 pagesSPE-177117-MS Learning by Impact Driving Training: A Case Study From EcuadorkomomoNo ratings yet
- Whole body vibration levels in urban bus driversDocument9 pagesWhole body vibration levels in urban bus driversmariaNo ratings yet
- Burgess Limerick 20229 ErgonomicsInterventionFinalReportJan2006Document93 pagesBurgess Limerick 20229 ErgonomicsInterventionFinalReportJan2006Eduardo JimenezNo ratings yet
- FBK AH MediTec 2016Document7 pagesFBK AH MediTec 2016fofuchinho mphili mphumapoNo ratings yet
- CE (Ra1) F (SK) PF1 (SHG SL) PFA (SHG KM) PN (KM)Document5 pagesCE (Ra1) F (SK) PF1 (SHG SL) PFA (SHG KM) PN (KM)MetinNo ratings yet
- Work-Related Road Safety: A Review of The Evidence For InterventionsDocument12 pagesWork-Related Road Safety: A Review of The Evidence For InterventionsUmairNo ratings yet
- Fatigue Detection For Vehicle Monitoring Using Computer VisionDocument12 pagesFatigue Detection For Vehicle Monitoring Using Computer VisionInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- Investigating The Influence of DistDocument11 pagesInvestigating The Influence of Distshariifcqaadir985No ratings yet
- Short Report Fatigue and The Road Users: Travellers' Account!Document10 pagesShort Report Fatigue and The Road Users: Travellers' Account!balan.anca2857No ratings yet
- CDC 5345 DS1Document150 pagesCDC 5345 DS1FioriAmeliaHathawayNo ratings yet
- 1 s2.0 S2351978915005600 MainDocument8 pages1 s2.0 S2351978915005600 MainhilmaNo ratings yet
- Spanish Profit Shifting Impact on Tax RevenueDocument13 pagesSpanish Profit Shifting Impact on Tax RevenuePatrickBernardoNo ratings yet
- Driving Simulation For Evaluation and Rehabilitation of Driving After StrokeDocument9 pagesDriving Simulation For Evaluation and Rehabilitation of Driving After StrokeMar Ruiz CuadraNo ratings yet
- Ergonomic Risk Assessment A Case Study of A Garment Manufacturing IndustryDocument7 pagesErgonomic Risk Assessment A Case Study of A Garment Manufacturing IndustryJOSE JAVIER BARZALLO GALVEZNo ratings yet
- Indian J CVCDocument17 pagesIndian J CVCagacheugen6335No ratings yet
- Design and Evaluation of Ergonomic Interventions For The Prevention of Musculoskeletal Disorders in IndiaDocument7 pagesDesign and Evaluation of Ergonomic Interventions For The Prevention of Musculoskeletal Disorders in IndiaRenaldiPrimaSaputraNo ratings yet
- Erratum To: Comparative Assessment of Physical and Cognitive Ergonomics Associated With Robotic and Traditional Laparoscopic SurgeriesDocument11 pagesErratum To: Comparative Assessment of Physical and Cognitive Ergonomics Associated With Robotic and Traditional Laparoscopic Surgeriesexpert 60No ratings yet
- DR Rashid FarooquiDocument22 pagesDR Rashid Farooquiqudsiatahniyath123No ratings yet
- Effectiveness of An Improved Road Safety Policy in EthiopiaDocument6 pagesEffectiveness of An Improved Road Safety Policy in EthiopiatilahunNo ratings yet
- References ErgoDocument13 pagesReferences ErgomizanNo ratings yet
- 145 762 1 PBDocument5 pages145 762 1 PBlishaNo ratings yet
- Reviewing In-Vehicle Systems To Improve Fuel Efficiency and Road SafetyDocument8 pagesReviewing In-Vehicle Systems To Improve Fuel Efficiency and Road SafetyMOBILE LEGENDS GENIUS MOMENTSNo ratings yet
- Sustainability DevelopmentDocument12 pagesSustainability DevelopmentVishal MehtaNo ratings yet
- Sustainability 12 01971Document12 pagesSustainability 12 01971Vishal MehtaNo ratings yet
- Mansur 2016 IOP Conf. Ser. Mater. Sci. Eng. 105 012033Document10 pagesMansur 2016 IOP Conf. Ser. Mater. Sci. Eng. 105 012033Fahmi MatarangNo ratings yet
- Ferreira ACE-R Accident Analysis 12Document10 pagesFerreira ACE-R Accident Analysis 12Ana VanessaNo ratings yet
- Fall ArestDocument22 pagesFall ArestAli RizviNo ratings yet
- An observational method for Postural Ergonomic Risk Assessment (PERA)Document19 pagesAn observational method for Postural Ergonomic Risk Assessment (PERA)ttorrespoNo ratings yet
- Wiegand 2009Document7 pagesWiegand 2009rulas workNo ratings yet
- JURDING 1 - Usefulness of Lung Ultrasound For Early Detection of Hospital-Acquired Pneumonia in Cardiac Critically Ill Patients On Venoarterial Extracorporeal Membrane OxygenationDocument10 pagesJURDING 1 - Usefulness of Lung Ultrasound For Early Detection of Hospital-Acquired Pneumonia in Cardiac Critically Ill Patients On Venoarterial Extracorporeal Membrane OxygenationLivia Meidy UbayidNo ratings yet
- Acquired HemophiliaDocument11 pagesAcquired HemophiliaLivia Meidy UbayidNo ratings yet
- 10.1186@s13054 020 03091 2 PDFDocument13 pages10.1186@s13054 020 03091 2 PDFJuan Jose SantivañezNo ratings yet
- AKI in Hospitalized Patients With COVID-19: Clinical ResearchDocument32 pagesAKI in Hospitalized Patients With COVID-19: Clinical ResearchLivia Meidy UbayidNo ratings yet
- Revisiting Hemophilia Management in Acute MedicineDocument6 pagesRevisiting Hemophilia Management in Acute MedicineLivia Meidy UbayidNo ratings yet
- Human Kidney Is A Target For Novel Severe Acute Respiratory Syndrome Coronavirus 2 InfectionDocument9 pagesHuman Kidney Is A Target For Novel Severe Acute Respiratory Syndrome Coronavirus 2 InfectionLivia Meidy UbayidNo ratings yet
- JURDING 2 - Update of The Treatment of Nosocomial Pneumonia in The ICUDocument13 pagesJURDING 2 - Update of The Treatment of Nosocomial Pneumonia in The ICULivia Meidy UbayidNo ratings yet
- JURDING 3 - Influencing Factors of Hospital-Acquired Pneumonia Infection in The Middle-Aged and Elderly Patients With SchizophreniaDocument7 pagesJURDING 3 - Influencing Factors of Hospital-Acquired Pneumonia Infection in The Middle-Aged and Elderly Patients With SchizophreniaLivia Meidy UbayidNo ratings yet
- Seizure Freedom After Laser Amygdalohippocampotomy Guided by Bilateral Responsive Neurostimulation in Pediatric Epilepsy: Illustrative CaseDocument5 pagesSeizure Freedom After Laser Amygdalohippocampotomy Guided by Bilateral Responsive Neurostimulation in Pediatric Epilepsy: Illustrative CaseLivia Meidy UbayidNo ratings yet
- Systematic Review of COVID-19 in Children Shows Milder Cases and A Better Prognosis Than AdultsDocument8 pagesSystematic Review of COVID-19 in Children Shows Milder Cases and A Better Prognosis Than AdultsLivia Meidy UbayidNo ratings yet
- Acute Kidney Injury: 2018 Usrds Annual Data Report - Volume 1: CKD in The United States 99Document26 pagesAcute Kidney Injury: 2018 Usrds Annual Data Report - Volume 1: CKD in The United States 99Livia Meidy UbayidNo ratings yet
- Aki Study Perbandingan Covid N NonDocument25 pagesAki Study Perbandingan Covid N Nonyesa m.sNo ratings yet
- Clinical Characteristics, Treatment and Outcomes of Paediatric COVID-19: A Systematic Review and Meta-AnalysisDocument9 pagesClinical Characteristics, Treatment and Outcomes of Paediatric COVID-19: A Systematic Review and Meta-AnalysisLivia Meidy UbayidNo ratings yet
- 2020 Wang - Clinical Characteristics of 138 Hospitalized PatientsDocument9 pages2020 Wang - Clinical Characteristics of 138 Hospitalized Patientsusman dilawarNo ratings yet
- The RIFLE and AKIN Classifications For Acute Kidney Injury: A Critical and Comprehensive ReviewDocument7 pagesThe RIFLE and AKIN Classifications For Acute Kidney Injury: A Critical and Comprehensive ReviewLivia Meidy UbayidNo ratings yet
- CC 4915Document10 pagesCC 4915Livia Meidy UbayidNo ratings yet
- The Rise of Prevalence and The Fall of Mortality of Patients With Acute Renal Failure: What The Analysis of Two Databases Does and Does Not Tell UsDocument3 pagesThe Rise of Prevalence and The Fall of Mortality of Patients With Acute Renal Failure: What The Analysis of Two Databases Does and Does Not Tell UsLivia Meidy UbayidNo ratings yet
- Guidance For Clinicians Managing Children at Risk Of, or With, Acute Kidney InjuryDocument14 pagesGuidance For Clinicians Managing Children at Risk Of, or With, Acute Kidney InjuryLivia Meidy UbayidNo ratings yet
- Research LetterDocument2 pagesResearch LetterLivia Meidy UbayidNo ratings yet
- Peritoneal Dialysis Treatment in Small Children With Acute Kidney Injury: Experience in Northwest ChinaDocument6 pagesPeritoneal Dialysis Treatment in Small Children With Acute Kidney Injury: Experience in Northwest ChinaLivia Meidy UbayidNo ratings yet
- Faktor Risiko Musculoskeletal Disorders (MSDS) Pada Pekerja Tenun Ikat Di Kelurahan Tuan Kentang Kota PalembangDocument10 pagesFaktor Risiko Musculoskeletal Disorders (MSDS) Pada Pekerja Tenun Ikat Di Kelurahan Tuan Kentang Kota PalembangChelvin oppierNo ratings yet
- Public Health Perspectives Journal: Asyhara Naela Arifin, Asih Kuswardinah, Sri Maryati DelianaDocument8 pagesPublic Health Perspectives Journal: Asyhara Naela Arifin, Asih Kuswardinah, Sri Maryati DelianaLivia Meidy UbayidNo ratings yet
- Physics Investigatory Project Class 12Document12 pagesPhysics Investigatory Project Class 12shivanginirai7No ratings yet
- CH 2Document20 pagesCH 2Vivek SinghNo ratings yet
- Trisyl Silica Gel: For Oils/Fats and Biofuel RefiningDocument4 pagesTrisyl Silica Gel: For Oils/Fats and Biofuel RefiningJosé Mauricio Bonilla TobónNo ratings yet
- Mcimt NDT Kids at 1Document12 pagesMcimt NDT Kids at 1api-485106673No ratings yet
- OTC Drug ListDocument7 pagesOTC Drug ListHong Diem100% (1)
- Modified Pfirrmann Grading System For Lumbar Intervertebral Disc DegenerationDocument6 pagesModified Pfirrmann Grading System For Lumbar Intervertebral Disc DegenerationZack StylesNo ratings yet
- Amul India Case Study: Product Portfolio and SWOT AnalysisDocument10 pagesAmul India Case Study: Product Portfolio and SWOT AnalysisShruti NagmoteNo ratings yet
- Hydrostatic Testing ProcedureDocument21 pagesHydrostatic Testing ProcedureFerdie OSNo ratings yet
- Radio Frequency Field - Bioeffects & SafetyDocument37 pagesRadio Frequency Field - Bioeffects & SafetyAmel AntonyNo ratings yet
- Master Key Bonus - The Healing CodeDocument8 pagesMaster Key Bonus - The Healing CodeChanterelle Vasto100% (12)
- NCERT Class 6 Geography Chapter 1 YouTube Lecture HandoutsDocument5 pagesNCERT Class 6 Geography Chapter 1 YouTube Lecture Handoutskalasri100% (1)
- April 12th Test PDFDocument32 pagesApril 12th Test PDFهخه •No ratings yet
- Wheat Sourdough Fermentation - Effects of Time and Acidification On Fundamental Rheological PropertiesDocument9 pagesWheat Sourdough Fermentation - Effects of Time and Acidification On Fundamental Rheological PropertiesmaurodiloretoNo ratings yet
- Sound Level MeterDocument11 pagesSound Level MeterFityatal HasanahNo ratings yet
- Guided Noteboo Kin GED10 2 (Mathe Matics in The Modern World)Document5 pagesGuided Noteboo Kin GED10 2 (Mathe Matics in The Modern World)Chenie BatacNo ratings yet
- A 1116Document15 pagesA 1116Rama S. SinghNo ratings yet
- Implementation of Swachh Bharat in MysoreDocument13 pagesImplementation of Swachh Bharat in MysoreDipyaman ChoudhuryNo ratings yet
- Appendix VIII - Civil and Structural Scope of WorkDocument140 pagesAppendix VIII - Civil and Structural Scope of WorkjaganrajNo ratings yet
- Candidates applied for Medical Officer post on contract basisDocument11 pagesCandidates applied for Medical Officer post on contract basiszephyrNo ratings yet
- A4 RelationshipgridDocument32 pagesA4 RelationshipgridjamesNo ratings yet
- EWC661 TITLE: Dietary Habits During Term Time Among University Students. Background of StudyDocument4 pagesEWC661 TITLE: Dietary Habits During Term Time Among University Students. Background of StudyfarinaazmiNo ratings yet
- Business Plan Hair DyeDocument12 pagesBusiness Plan Hair Dyercool_rahul0039341No ratings yet
- NCM 106 Acute Biologic CrisisDocument142 pagesNCM 106 Acute Biologic CrisisEllamae Chua88% (8)
- Apcosil 605Document1 pageApcosil 605rihtak123No ratings yet
- Psychedelic Drugs-A New Era in Psychiatry?Document9 pagesPsychedelic Drugs-A New Era in Psychiatry?PeterNo ratings yet
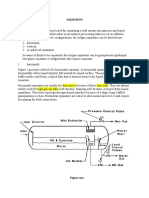
- Separators: Figure OneDocument8 pagesSeparators: Figure OneMohamed Moder100% (1)
- SEN Code of Practice 2001Document148 pagesSEN Code of Practice 2001Matt GrantNo ratings yet
- Symbol High Low R5 R4 R3 R2: DailyDocument8 pagesSymbol High Low R5 R4 R3 R2: Daily257597 rmp.mech.16No ratings yet
- English Sds Turalik 52Document13 pagesEnglish Sds Turalik 52Muhammad ArifudinNo ratings yet
- Substrates P400 enDocument111 pagesSubstrates P400 enLince WijoyoNo ratings yet