You might also like
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- OB - Cardiovascular Disorders (LRA)Document6 pagesOB - Cardiovascular Disorders (LRA)Anonymous ANo ratings yet
- Pedia Cardio Lecture AidDocument5 pagesPedia Cardio Lecture AidStephanie Pearl AldaNo ratings yet
- Congenital Heart DiseaseDocument8 pagesCongenital Heart DiseaseSanthosh.S.U100% (3)
- Pediatric Cardiology Part 2Document3 pagesPediatric Cardiology Part 2carlosNo ratings yet
- Cardiac DisordersDocument81 pagesCardiac DisordersCarias Baby AnnNo ratings yet
- Disturbances in CirculationDocument12 pagesDisturbances in CirculationJoei OcampoNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFRuval PhenexNo ratings yet
- Kuliah Kriris HTDocument29 pagesKuliah Kriris HTDiska irmadhaniNo ratings yet
- Cardiomyopathy PathogenesisDocument3 pagesCardiomyopathy PathogenesisThrift AdvisoryNo ratings yet
- Pulmonary Embolism Diagnosis and TreatmentDocument29 pagesPulmonary Embolism Diagnosis and TreatmentCommandoCitotz100% (1)
- Pathophysiology of Congestive Heart FailureDocument3 pagesPathophysiology of Congestive Heart FailureMel Izhra N. MargateNo ratings yet
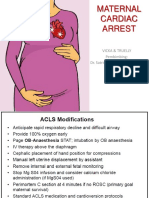
- Maternal Cardiac ArrestDocument28 pagesMaternal Cardiac ArrestTruelly ChanantaNo ratings yet
- 1 CHFDocument62 pages1 CHFFalmeta EliyasNo ratings yet
- PY6030 Term 1Document13 pagesPY6030 Term 1AlexaJoiceJumao-AsNo ratings yet
- Isue October 2011intensivistneonatalandpediartriccardiacemergenciesDocument6 pagesIsue October 2011intensivistneonatalandpediartriccardiacemergenciesSaif HashimNo ratings yet
- 4.18 Mankad Echo in Systemic DiseaseDocument97 pages4.18 Mankad Echo in Systemic DiseaseDiana_anca6No ratings yet
- Pre Gestational 1Document12 pagesPre Gestational 1Fatima TañedoNo ratings yet
- TOF Pathophysiology and TreatmentDocument4 pagesTOF Pathophysiology and TreatmentDoreen Claire M. WallangNo ratings yet
- CHF & CardiomyopathiesDocument25 pagesCHF & CardiomyopathiesDan HoNo ratings yet
- 7 Congestive Heart FailureDocument13 pages7 Congestive Heart FailureVictor PazNo ratings yet
- Cardiac Diseases in PregnancyDocument27 pagesCardiac Diseases in PregnancyHoney May Rollan Vicente50% (2)
- Ischemic Heart DiseaseDocument28 pagesIschemic Heart DiseaseLiusHarimanNo ratings yet
- Table Summary of RisksDocument2 pagesTable Summary of RisksAlyson DrewNo ratings yet
- High Risk AdultDocument7 pagesHigh Risk AdultJen IlaganNo ratings yet
- Taponamiento CardiacoDocument9 pagesTaponamiento CardiacoLiz Aliaga KnutzenNo ratings yet
- Module No. Date: Topic:: Cues/Questions/ Keywords Notes Congenital Heart DisordersDocument28 pagesModule No. Date: Topic:: Cues/Questions/ Keywords Notes Congenital Heart Disordersanon ymousNo ratings yet
- Hi-Yield Notes in Im & PediaDocument20 pagesHi-Yield Notes in Im & PediaJohn Christopher LucesNo ratings yet
- Pathophysiology of Congestive Heart Failure: Predisposing Factors Precipitating/Aggravating FactorsDocument1 pagePathophysiology of Congestive Heart Failure: Predisposing Factors Precipitating/Aggravating Factorsguillermojerry100% (2)
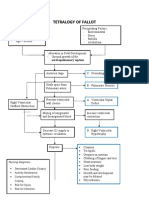
- Tetralogy of Fallot Pathophysiology & Risk FactorsDocument1 pageTetralogy of Fallot Pathophysiology & Risk FactorsEiztirfNo ratings yet
- Supan-Clinical Case AnalysisDocument7 pagesSupan-Clinical Case AnalysisAjay SupanNo ratings yet
- AnnCardAnaesth10119-300904 082130 PDFDocument8 pagesAnnCardAnaesth10119-300904 082130 PDFFirah Triple'sNo ratings yet
- AcyanoticDocument3 pagesAcyanotic2AAQUINO, PRECIOUS ANGEL F.No ratings yet
- Cardio My Opa Thies ChartDocument2 pagesCardio My Opa Thies ChartSolomon Seth SallforsNo ratings yet
- Surgery II: Congenital Heart DiseaseDocument10 pagesSurgery II: Congenital Heart DiseaseRea Dominique CabanillaNo ratings yet
- ShockDocument39 pagesShockCut Ristina OlviaNo ratings yet
- Angina Pect & Infark Miokard (Dr. Ilham Uddin, SP - JP (K) )Document108 pagesAngina Pect & Infark Miokard (Dr. Ilham Uddin, SP - JP (K) )Vania Nazhara FitrianaNo ratings yet
- Pathophysiology of Ventricular Septal DefectsDocument3 pagesPathophysiology of Ventricular Septal DefectsJessa NodaloNo ratings yet
- Pathophysiology of Congenital Heart DiseasesDocument8 pagesPathophysiology of Congenital Heart DiseaseskishanNo ratings yet
- Pathophysiology of Congenital Heart Diseases PDFDocument8 pagesPathophysiology of Congenital Heart Diseases PDFdramitjainNo ratings yet
- Cardiogenic Shock Dr. ArieDocument40 pagesCardiogenic Shock Dr. Arierio kristianNo ratings yet
- PT Management & Problems of The CV System - Part 4 Cheat SheetDocument2 pagesPT Management & Problems of The CV System - Part 4 Cheat SheetKat KatNo ratings yet
- Heart disease in pregnancyDocument87 pagesHeart disease in pregnancyMonisha ArulalanNo ratings yet
- ACC Jimmy AsafDocument152 pagesACC Jimmy AsafFikriYTNo ratings yet
- Atrial FibrillationDocument1 pageAtrial FibrillationRizia Emery SwedberghNo ratings yet
- B. Create Your Concept Map of The Disorder. Use A Separate Paper For This. Use Short Coupon Bond and Draw Your Concept Map Using This FormatDocument5 pagesB. Create Your Concept Map of The Disorder. Use A Separate Paper For This. Use Short Coupon Bond and Draw Your Concept Map Using This FormatPatricia Jean FaeldoneaNo ratings yet
- Tetralogy of Fallot Nursing Diagnosis and ManagementDocument2 pagesTetralogy of Fallot Nursing Diagnosis and ManagementKarl KiwisNo ratings yet
- Pa 02 CardioDocument45 pagesPa 02 CardioElly NuñezNo ratings yet
- Outcome Pada Penyakit Jantung Terhadap Ibu Dan Janin Selama KehamilanDocument28 pagesOutcome Pada Penyakit Jantung Terhadap Ibu Dan Janin Selama KehamilanRaras PraminingrumNo ratings yet
- Algoritma Nyeri Dada - Dian WDocument4 pagesAlgoritma Nyeri Dada - Dian WfaberNo ratings yet
- Stoelting Anasthesia and Co Existing Disease PDFDocument28 pagesStoelting Anasthesia and Co Existing Disease PDFEgidia SetyaNo ratings yet
- ACS Management GuideDocument18 pagesACS Management GuideYadah IkamNo ratings yet
- Emd1-K22-Cardiac EmergencyDocument49 pagesEmd1-K22-Cardiac EmergencyAnanta GintingNo ratings yet
- Atrial FibrillationDocument24 pagesAtrial FibrillationsatriaNo ratings yet
- 2 CardioDocument2 pages2 Cardiolouise VincoNo ratings yet
- Atrial Septal DefectDocument4 pagesAtrial Septal Defectlittle miss scare-allNo ratings yet
- Clinical Case Analysis: Tarlac State University College of ScienceDocument3 pagesClinical Case Analysis: Tarlac State University College of ScienceKrisianne Mae Lorenzo FranciscoNo ratings yet
- Nursing Care of Stroke - NewDocument4 pagesNursing Care of Stroke - Newninda saputriNo ratings yet
- THYROID GLAND: What Happens When Something Goes Wrong?: PIT UIDocument4 pagesTHYROID GLAND: What Happens When Something Goes Wrong?: PIT UIAnonymous HH3c17osNo ratings yet
- Obstetrics Pulmonary Diseases During Pregnancy: Clinical StagesDocument2 pagesObstetrics Pulmonary Diseases During Pregnancy: Clinical StagesAnonymous HH3c17osNo ratings yet
- Instapay Ach Participants: Sender/Receiver Receiver OnlyDocument1 pageInstapay Ach Participants: Sender/Receiver Receiver OnlyAnonymous HH3c17osNo ratings yet
- Wheezing SmokeDocument3 pagesWheezing SmokeAnonymous HH3c17osNo ratings yet
- The Study of Business and The LikeDocument49 pagesThe Study of Business and The LikeAnonymous HH3c17osNo ratings yet
- Project ReadingDocument28 pagesProject ReadingAnonymous HH3c17osNo ratings yet
- US V Ah ChongDocument3 pagesUS V Ah ChongAnonymous HH3c17osNo ratings yet
- PSE listed companies instrumentsDocument4 pagesPSE listed companies instrumentsAnonymous HH3c17osNo ratings yet
- Uptodate AppendicitisDocument28 pagesUptodate AppendicitisAnonymous HH3c17osNo ratings yet
- Taxation of judicial salariesDocument2 pagesTaxation of judicial salariesAnonymous HH3c17osNo ratings yet
- Confidence IDocument4 pagesConfidence IAnonymous HH3c17osNo ratings yet
- When Law Takes Effect: Chapter 6: Official GazetteDocument4 pagesWhen Law Takes Effect: Chapter 6: Official GazetteAnonymous HH3c17osNo ratings yet
- 228 B.M. 1625 Uy TimosaDocument2 pages228 B.M. 1625 Uy TimosaAnonymous HH3c17osNo ratings yet
- Corporate Governance and Finance Department: Issuer of Proprietary/Non-Proprietary Shares/CertificatesDocument3 pagesCorporate Governance and Finance Department: Issuer of Proprietary/Non-Proprietary Shares/CertificatesAnonymous HH3c17osNo ratings yet
- Your HEXACO-PI-R Results: Warning: Your Results Are Very Likely Invalid Due To Inattentive RespondingDocument6 pagesYour HEXACO-PI-R Results: Warning: Your Results Are Very Likely Invalid Due To Inattentive RespondingMichael John BegalmeNo ratings yet
- Persons Notes AgainDocument6 pagesPersons Notes AgainAnonymous HH3c17osNo ratings yet
- Laz HernandDocument41 pagesLaz HernandAnonymous HH3c17osNo ratings yet
- Supreme Court Justice who resisted MarcosDocument1 pageSupreme Court Justice who resisted MarcosAnonymous HH3c17osNo ratings yet
- AngaraDocument4 pagesAngaraAnonymous HH3c17osNo ratings yet
- Self Measures For Self-Esteem Rosenberg Self-EsteemDocument4 pagesSelf Measures For Self-Esteem Rosenberg Self-Esteemapi-349021587No ratings yet
- Sere Not A DigestDocument4 pagesSere Not A DigestAnonymous HH3c17osNo ratings yet
- Not A Car DigesDocument3 pagesNot A Car DigesAnonymous HH3c17osNo ratings yet
- AngaraDocument4 pagesAngaraAnonymous HH3c17osNo ratings yet
- TableDocument7 pagesTableAnonymous HH3c17osNo ratings yet
- SummaryDocument3 pagesSummaryAnonymous HH3c17osNo ratings yet
- DIGEST - UCPB v. Uy, G.R. No. 204039 PDFDocument2 pagesDIGEST - UCPB v. Uy, G.R. No. 204039 PDFAnonymous HH3c17os50% (2)
- The Digest of The Com andDocument2 pagesThe Digest of The Com andAnonymous HH3c17osNo ratings yet
- Mistake of Fact Defense Rejected in 1943 Murder CaseDocument2 pagesMistake of Fact Defense Rejected in 1943 Murder CaseAnonymous HH3c17osNo ratings yet
- Mistake of Fact Defense Rejected in 1943 Murder CaseDocument2 pagesMistake of Fact Defense Rejected in 1943 Murder CaseAnonymous HH3c17osNo ratings yet
- Trauma Dan Kegawatdaruratan MataDocument92 pagesTrauma Dan Kegawatdaruratan MataM Isyhaduul IslamNo ratings yet
- Magic MouthwashDocument5 pagesMagic MouthwashAdiAri Rosiu100% (3)
- Chapter 04 Individual Values Perceptions and Reactions: TruefalseDocument27 pagesChapter 04 Individual Values Perceptions and Reactions: Truefalseboerd77No ratings yet
- Pregnancy Risk Assessment Forms HSEJuly 2015 PDFDocument5 pagesPregnancy Risk Assessment Forms HSEJuly 2015 PDFAndrei Razvan GasparelNo ratings yet
- Cesar - Evaluation - ImciDocument3 pagesCesar - Evaluation - ImcikdfhjfhfNo ratings yet
- #591 Lot.85730 EinsertDocument2 pages#591 Lot.85730 Einsertjnyng222No ratings yet
- Safety Data Sheet (SDS) Anysol-D100Document11 pagesSafety Data Sheet (SDS) Anysol-D100U.s. Ezhil ArivudainambiNo ratings yet
- This Is Lean PDFDocument49 pagesThis Is Lean PDFMisael50% (2)
- Micro Teaching On: Placenta PreviaDocument10 pagesMicro Teaching On: Placenta Previasuchismita pandaNo ratings yet
- Taking Medical HistoryDocument2 pagesTaking Medical HistoryDiana KulsumNo ratings yet
- Social Science & Medicine: Phil Brown, Mercedes Lyson, Tania JenkinsDocument5 pagesSocial Science & Medicine: Phil Brown, Mercedes Lyson, Tania JenkinsVivian DiazNo ratings yet
- CBD HepatomaDocument201 pagesCBD HepatomafaridNo ratings yet
- 25 30ijpdtDocument7 pages25 30ijpdtSalsa BilaNo ratings yet
- Review of Literature On Breast Self Examination in IndiaDocument8 pagesReview of Literature On Breast Self Examination in Indiac5m82v4xNo ratings yet
- Interpretation of Laboratory Thyroid Function Tests: The "Hidden" Health ProblemDocument38 pagesInterpretation of Laboratory Thyroid Function Tests: The "Hidden" Health Problemalanoud.877No ratings yet
- Exercise 6 Make An Incident Report and Conduct An InvestigationDocument5 pagesExercise 6 Make An Incident Report and Conduct An InvestigationRoxana BaltatescuNo ratings yet
- NeurologyDocument23 pagesNeurologyAhmad Naufal Basri100% (3)
- Undergraduate Research Proposal FormDocument50 pagesUndergraduate Research Proposal FormMaria Carmela Rachel GazilNo ratings yet
- SLE Case Report on 15-Year-Old GirlDocument38 pagesSLE Case Report on 15-Year-Old GirlDiLa NandaRiNo ratings yet
- NeuroLink Stent SystemDocument16 pagesNeuroLink Stent SystemneureportNo ratings yet
- Projective Tests GuideDocument35 pagesProjective Tests GuideHera FakherNo ratings yet
- Nursing Documentation WorkshopDocument6 pagesNursing Documentation WorkshopJulie AnnNo ratings yet
- B.SC Nursing 3rd Year SyllabusDocument53 pagesB.SC Nursing 3rd Year SyllabusSooraj Krishna sNo ratings yet
- Peterson Practice Test 2 SatDocument46 pagesPeterson Practice Test 2 SatAiko EugeniaNo ratings yet
- Drug Study: St. Joseph CollegeDocument3 pagesDrug Study: St. Joseph CollegeeninajerhicaNo ratings yet
- Pharmacist's Cheat Sheet For Obese Patients: I. ObesityDocument6 pagesPharmacist's Cheat Sheet For Obese Patients: I. ObesityArchie CabacheteNo ratings yet
- Physical and Healthy ImpairmentsDocument27 pagesPhysical and Healthy ImpairmentsMwanalushi KanjalaNo ratings yet
- RTC RulingDocument3 pagesRTC RulingLeeNo ratings yet
- H2O2 Nebulization Therapy 3.19.2020Document5 pagesH2O2 Nebulization Therapy 3.19.2020Theodosius Arcadius100% (1)
- 3-Sumran Ali, MPA (Hefei-China) PDFDocument16 pages3-Sumran Ali, MPA (Hefei-China) PDFWahyu WibowoNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)