You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Sistematika Radiologi Tulang Pada Kasus FrakturDocument3 pagesSistematika Radiologi Tulang Pada Kasus FrakturBrando PanjaitanNo ratings yet
- 1 s2.0 S1110184914000634 MainDocument4 pages1 s2.0 S1110184914000634 MainBrando PanjaitanNo ratings yet
- Management of Eyelid Lacerations: CornerDocument6 pagesManagement of Eyelid Lacerations: CornerBrando PanjaitanNo ratings yet
- Case Report: Anesthetic Management of Acute Fatty Liver of Pregnancy in The Postpartum PeriodDocument6 pagesCase Report: Anesthetic Management of Acute Fatty Liver of Pregnancy in The Postpartum PeriodBrando PanjaitanNo ratings yet
- Methylprednisolone Vs Dexamethasone For Control VertigoDocument8 pagesMethylprednisolone Vs Dexamethasone For Control VertigoBrando PanjaitanNo ratings yet
- Zephyr/Venezia Range Hood ManualDocument14 pagesZephyr/Venezia Range Hood Manualfandy15No ratings yet
- Design of Machine Elements: Prof. Sujatha SrinivasanDocument27 pagesDesign of Machine Elements: Prof. Sujatha Srinivasanraviraj kumarNo ratings yet
- The Philippine Informal Reading InventoryDocument2 pagesThe Philippine Informal Reading InventoryVenilyn Cruz91% (11)
- F 8 T 161 P 960 N 1Document7 pagesF 8 T 161 P 960 N 1Jessica PratesNo ratings yet
- Lab 9Document3 pagesLab 9Tâm NguyễnNo ratings yet
- Ce 8 Sem Advanced Reinforced Cement Concrete Design Winter 2018Document2 pagesCe 8 Sem Advanced Reinforced Cement Concrete Design Winter 2018SandeepNo ratings yet
- C6-Cable1-2 LSSS-LN0090-01 (UTP C6 - 250MHz)Document6 pagesC6-Cable1-2 LSSS-LN0090-01 (UTP C6 - 250MHz)crisandy31No ratings yet
- Imanager U2000 ME Release Notes 01 PDFDocument180 pagesImanager U2000 ME Release Notes 01 PDFCamilo Andres OrozcoNo ratings yet
- Factors Affecting Internal Resistance em 1587263355Document12 pagesFactors Affecting Internal Resistance em 1587263355SHIBU PRASAD SAHOO100% (1)
- ADL 12 Business Laws V4Document26 pagesADL 12 Business Laws V4Aditya BhatNo ratings yet
- JVC HR-S6970AA Service ManualDocument61 pagesJVC HR-S6970AA Service ManualPriyantha GanegodaNo ratings yet
- Bài Kt 2 Biên Dịch 1-LiêmDocument10 pagesBài Kt 2 Biên Dịch 1-LiêmNguyen Loan100% (1)
- E-Katalog Warna - FullDocument43 pagesE-Katalog Warna - Fullarend alfiyantoNo ratings yet
- Pit Installations - Restricted Airflow SituationsDocument16 pagesPit Installations - Restricted Airflow Situationsfarshan296015No ratings yet
- Adult Neurological QuestionnaireDocument1 pageAdult Neurological QuestionnaireIqbal BaryarNo ratings yet
- Beamray 50R100R Data SheetDocument2 pagesBeamray 50R100R Data Sheethassan elgamriNo ratings yet
- TSX Datasheet 2021 05Document10 pagesTSX Datasheet 2021 05Filipe LaínsNo ratings yet
- One Plus Case StudyDocument9 pagesOne Plus Case StudyShubham Shimpi50% (2)
- Accident Investigation Report: Investigator's InformationDocument2 pagesAccident Investigation Report: Investigator's InformationJack PNo ratings yet
- Freshers - HR Interview Questions at AccentureDocument3 pagesFreshers - HR Interview Questions at Accenturebtrecio03No ratings yet
- What Is OLAP? Cube, Operations & Types in Data WarehouseDocument7 pagesWhat Is OLAP? Cube, Operations & Types in Data WarehouseGabrielAlexandruNo ratings yet
- Annexure 5.14 BC Mix DesignDocument10 pagesAnnexure 5.14 BC Mix Designmiesty50% (2)
- Ambitious TheoryDocument14 pagesAmbitious TheoryPhanilla IceCreamNo ratings yet
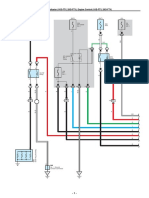
- ECT and A/T Indicator (1KD-FTV, 2KD-FTV), Engine Control (1KD-FTV, 2KD-FTV)Document33 pagesECT and A/T Indicator (1KD-FTV, 2KD-FTV), Engine Control (1KD-FTV, 2KD-FTV)Erick Lizana Neyra100% (4)
- Anti LeproticDocument9 pagesAnti LeproticMeenakshi shARMANo ratings yet
- For Students ModuleDocument44 pagesFor Students ModuleJohn vincent VellezaNo ratings yet
- SosDocument6 pagesSosVikramNo ratings yet
- Prs-021-0025 - C. Melchers - Coca Cola Naga ProjectDocument2 pagesPrs-021-0025 - C. Melchers - Coca Cola Naga ProjectMiko Christopher OroyanNo ratings yet
- SpainDocument3 pagesSpainSima MiliunaiteNo ratings yet
- Revealed Comparative AdvantageDocument5 pagesRevealed Comparative AdvantageiamrahulkumarNo ratings yet