You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Strategic Cost Management CabreraDocument5 pagesStrategic Cost Management CabreraJyrah Mae Aceron0% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Advertising Primer - J.P. Morgan PDFDocument141 pagesAdvertising Primer - J.P. Morgan PDFSacred WingsNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- MRP BajajDocument352 pagesMRP BajajRanesh Kumar0% (1)
- Chapter 5-Leadership and MotivationDocument62 pagesChapter 5-Leadership and MotivationAklilu GirmaNo ratings yet
- Case 3 Analysis AdtrackmediaDocument2 pagesCase 3 Analysis Adtrackmediaapi-526105414No ratings yet
- Telinga Hidung TenggorokanDocument111 pagesTelinga Hidung Tenggorokanharyo wiryantoNo ratings yet
- 5.6. Schematic - Bus Coupler-J2.10Document32 pages5.6. Schematic - Bus Coupler-J2.10Mèo Mập Ú NuNo ratings yet
- Interview For QualcommDocument3 pagesInterview For QualcommPratikshaKhade0% (1)
- Anatomy of Nose and Paranasal SinusDocument20 pagesAnatomy of Nose and Paranasal Sinusharyo wiryantoNo ratings yet
- Work Man 2017Document7 pagesWork Man 2017haryo wiryantoNo ratings yet
- Anatomy of The Throat DR Oscar PresentasiDocument53 pagesAnatomy of The Throat DR Oscar Presentasiharyo wiryantoNo ratings yet
- Is There An Association Between Migraine and Allergic Rhinitis?Document6 pagesIs There An Association Between Migraine and Allergic Rhinitis?haryo wiryantoNo ratings yet
- Case Dr. Oscar - Sinusitis1Document45 pagesCase Dr. Oscar - Sinusitis1haryo wiryantoNo ratings yet
- Foreign Body Aspiration in Infants and Older Children: A Comparative StudyDocument5 pagesForeign Body Aspiration in Infants and Older Children: A Comparative Studyharyo wiryantoNo ratings yet
- Association of Midlife Hypertension With Late-Life Hearing LossDocument8 pagesAssociation of Midlife Hypertension With Late-Life Hearing Lossharyo wiryantoNo ratings yet
- Leukoplakia or LPR The Misdiagnosis Orf Laryngeal TuberculosisDocument5 pagesLeukoplakia or LPR The Misdiagnosis Orf Laryngeal Tuberculosisharyo wiryantoNo ratings yet
- Postoperative Opioid Prescribing and Consumption Patterns After TonsillectomyDocument7 pagesPostoperative Opioid Prescribing and Consumption Patterns After Tonsillectomyharyo wiryantoNo ratings yet
- Depression in Patients With Tinnitus: A Systematic ReviewDocument8 pagesDepression in Patients With Tinnitus: A Systematic Reviewharyo wiryantoNo ratings yet
- Mandai2012 Article ClinicalManagementOfOvarianEndDocument17 pagesMandai2012 Article ClinicalManagementOfOvarianEndharyo wiryantoNo ratings yet
- Ford Ka Heater Fan Removal 1997 09Document3 pagesFord Ka Heater Fan Removal 1997 09Marius Dedal100% (1)
- The Arnolfini PortraitDocument2 pagesThe Arnolfini PortraitDragana RistovaNo ratings yet
- Physics MCQs For Class 12 With Answers Chapter 10Document12 pagesPhysics MCQs For Class 12 With Answers Chapter 10Akshith ReddyNo ratings yet
- Sentry 6000NEMA ESS DatasheetDocument8 pagesSentry 6000NEMA ESS Datasheetfandy mustafaNo ratings yet
- SMS2008 DX33Document4 pagesSMS2008 DX33Imam DinNo ratings yet
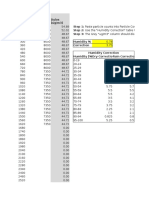
- Dylos Conversion Education - Cehs.health - Umt.eduDocument117 pagesDylos Conversion Education - Cehs.health - Umt.eduMCNo ratings yet
- Chapter Two Approaches To Ethics: Ayenew Birhanu (PHD)Document43 pagesChapter Two Approaches To Ethics: Ayenew Birhanu (PHD)Nasri IBRAHIMNo ratings yet
- Assignment 1-Vignesh Prasad VDocument14 pagesAssignment 1-Vignesh Prasad VVignesh Veera Prasad100% (1)
- PSA Wellness ProgramDocument39 pagesPSA Wellness ProgramFrannie PastorNo ratings yet
- S20191126coppercathodes Exdrc Lme 17 3Document3 pagesS20191126coppercathodes Exdrc Lme 17 3Engineer Anne MuthoniNo ratings yet
- A Dual-Linear Polarized Highly Isolated CrossedDocument4 pagesA Dual-Linear Polarized Highly Isolated CrossedPhạm GiangNo ratings yet
- The Amber Reside NC BrochureDocument12 pagesThe Amber Reside NC BrochureCheng Gi NiNo ratings yet
- Statistics in The Crem As of October 2020Document11 pagesStatistics in The Crem As of October 2020kamijou08No ratings yet
- Tendor of EsiDocument7 pagesTendor of EsiRaj KumarNo ratings yet
- Python Tkinter Grid GeometryDocument7 pagesPython Tkinter Grid GeometryPedro FigueiredoNo ratings yet
- Eaton Hydroline TS CylinderDocument8 pagesEaton Hydroline TS CylinderHanzil HakeemNo ratings yet
- Progress of Refractories Used in BFDocument8 pagesProgress of Refractories Used in BFAloísio Simões RibeiroNo ratings yet
- Sven Hoeger Case Study Habirshaw ParkDocument11 pagesSven Hoeger Case Study Habirshaw ParkRoberthothanNo ratings yet
- He Effect of AC (Alternating Current) and DC (Direct Current) On Bend Testing Results of Low Carbon Steel Welding JointsDocument6 pagesHe Effect of AC (Alternating Current) and DC (Direct Current) On Bend Testing Results of Low Carbon Steel Welding JointsIwankNo ratings yet
- Lyrics BLOODY MARYDocument1 pageLyrics BLOODY MARYMuhd Baqir AzidzNo ratings yet
- Hf1016414 Hoffman VentiladorDocument4 pagesHf1016414 Hoffman VentiladorMoises AlvarezNo ratings yet
- Chemical Industry in China-FinalDocument48 pagesChemical Industry in China-Finalsandeep_scNo ratings yet
- Question Paper Set I II NRM 121 2011 2Document4 pagesQuestion Paper Set I II NRM 121 2011 2hangkattesia82No ratings yet