You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Prostatitis: Symptoms, Causes and TreatmentsDocument16 pagesProstatitis: Symptoms, Causes and TreatmentsjoserodrrNo ratings yet
- Enlarged Prostate Booklet PDFDocument52 pagesEnlarged Prostate Booklet PDFnabin hamalNo ratings yet
- Male Reproductive SystemDocument37 pagesMale Reproductive SystemAzza100% (3)
- Gen Pathology CasesDocument41 pagesGen Pathology Casesrjh18950% (1)
- Ram ConceptDocument1,242 pagesRam ConceptYaserNo ratings yet
- Pourusha VastiDocument54 pagesPourusha Vastiksr prasadNo ratings yet
- Case Study On HypertensionDocument67 pagesCase Study On Hypertensiongideon A. owusu100% (3)
- What Causes Urinary Retention?Document4 pagesWhat Causes Urinary Retention?darkz_andreaslimNo ratings yet
- 364.16T-18 Physical Properties and Characteristics Affecting The Sensitivity To Cracking of Cementitious Repair Materials TechNoteDocument6 pages364.16T-18 Physical Properties and Characteristics Affecting The Sensitivity To Cracking of Cementitious Repair Materials TechNoteYaserNo ratings yet
- 222.3R-11 Guide To Design and Construction Practices To Mitigate Corrosion of Reinforcement in Concrete StructuresDocument32 pages222.3R-11 Guide To Design and Construction Practices To Mitigate Corrosion of Reinforcement in Concrete StructuresYaserNo ratings yet
- 364.5T-10 Importance of Modulus of Elasticity in Surface Repair Materials (TechNote)Document3 pages364.5T-10 Importance of Modulus of Elasticity in Surface Repair Materials (TechNote)YaserNo ratings yet
- 364.9T-03 (11) Cracks in A Repair (TechNote)Document3 pages364.9T-03 (11) Cracks in A Repair (TechNote)YaserNo ratings yet
- تاريخ الأمة القبطية - يعقوب نخلة روفيلةDocument422 pagesتاريخ الأمة القبطية - يعقوب نخلة روفيلةYaserNo ratings yet
- Pages From ICC 2015 IBC-2Document1 pagePages From ICC 2015 IBC-2YaserNo ratings yet
- Pages From 315R-18 Guide To Presenting Reinforcing Steel Design DetailsDocument1 pagePages From 315R-18 Guide To Presenting Reinforcing Steel Design DetailsYaserNo ratings yet
- FIGURE C26.5-1 Maximum Speed Averaged Over T S To Hourly Mean SpeedDocument2 pagesFIGURE C26.5-1 Maximum Speed Averaged Over T S To Hourly Mean SpeedYaser100% (1)
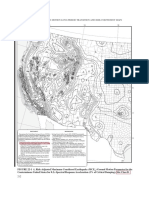
- Chapter 22 Seismic Ground Motion Long-Period Transition and Risk Coefficient MapsDocument6 pagesChapter 22 Seismic Ground Motion Long-Period Transition and Risk Coefficient MapsYaserNo ratings yet
- ETABS Concrete Frame Design: ACI 318-19 Column Section DesignDocument2 pagesETABS Concrete Frame Design: ACI 318-19 Column Section DesignYaserNo ratings yet
- Pages From AISC 303-2016Document1 pagePages From AISC 303-2016YaserNo ratings yet
- Comments ReferencesDocument4 pagesComments ReferencesYaserNo ratings yet
- Metod Base Cabinet For Built in Oven Sink - AA 2119848 1 - PubDocument40 pagesMetod Base Cabinet For Built in Oven Sink - AA 2119848 1 - PubYaserNo ratings yet
- F 60-1Document100 pagesF 60-1YaserNo ratings yet
- BPH NotesDocument6 pagesBPH NotesLorina ApelacioNo ratings yet
- Male Reproductive System and Female Reproductive SystemDocument8 pagesMale Reproductive System and Female Reproductive SystemLoriz DoronioNo ratings yet
- 10.male Reproductive System 2 BlocksDocument220 pages10.male Reproductive System 2 BlocksANA CAROLINE ANDRADE DE MELONo ratings yet
- Protoflow Reviews IS Legit 2023 Updated Report!Document9 pagesProtoflow Reviews IS Legit 2023 Updated Report!protoflow usaNo ratings yet
- Soal Try Out-2 Online Tbi 2018Document7 pagesSoal Try Out-2 Online Tbi 2018joyNo ratings yet
- Biology Project Class XIIDocument34 pagesBiology Project Class XIIBimal DasNo ratings yet
- Zinc, Copper and Selenium in ReproductionDocument15 pagesZinc, Copper and Selenium in ReproductionNéstor MirelesNo ratings yet
- 310-Article Text-582-1-10-20210312-1Document13 pages310-Article Text-582-1-10-20210312-1Ni Putu SwastyNo ratings yet
- Surgery ObjDocument66 pagesSurgery Objmintahmeshackbenjamin0% (1)
- DR Zadul - BPHDocument16 pagesDR Zadul - BPHVika IkaNo ratings yet
- Transurethral Resection of The Prostate (TURP)Document16 pagesTransurethral Resection of The Prostate (TURP)Princess Brigitte R. PATE�ANo ratings yet
- Histology of Seminal Vesicles & ProstateDocument22 pagesHistology of Seminal Vesicles & ProstateRafique AhmedNo ratings yet
- Urology IDocument34 pagesUrology IEbraheam HadiNo ratings yet
- Abstract Book Asmiua 2022Document203 pagesAbstract Book Asmiua 2022Lutfi Aulia RahmanNo ratings yet
- Health The Basics Canadian 6th Edition Donatelle Test BankDocument49 pagesHealth The Basics Canadian 6th Edition Donatelle Test Bankpucelleheliozoa40wo100% (22)
- Premature Ejaculation Treatment Burki, S Manoeuvre PDFDocument12 pagesPremature Ejaculation Treatment Burki, S Manoeuvre PDFarslanahmedkhawajaNo ratings yet
- Imaging of The Reproductive SystemDocument15 pagesImaging of The Reproductive SystemAbi SulitNo ratings yet
- Resarch UpdatedDocument48 pagesResarch Updatedapi-210258673No ratings yet
- Benigna Hiperplasia ProstatDocument23 pagesBenigna Hiperplasia ProstatShanti ArianiNo ratings yet
- Physical Examination of The 4 Genitourinary TractDocument12 pagesPhysical Examination of The 4 Genitourinary TractrudybisNo ratings yet
- The Reproductive System The Reproductive System: © 2018 Pearson Education, Ltd. 1Document19 pagesThe Reproductive System The Reproductive System: © 2018 Pearson Education, Ltd. 1lourd nabNo ratings yet
- Chronic Prostatitis A Possible Cause of HematospermiaDocument6 pagesChronic Prostatitis A Possible Cause of HematospermiaZlatan ZvizdicNo ratings yet
- Medical Dictionary Letter DDocument6 pagesMedical Dictionary Letter DjnelbmbaNo ratings yet