You might also like
- Synthesis PaperDocument8 pagesSynthesis Paperapi-403776891No ratings yet
- Ebp Formative Synthesis PaperDocument9 pagesEbp Formative Synthesis Paperapi-404415990No ratings yet
- The Efficacy of Daily Chlorhexidine Bathing For Preventing Healthcare-Associated Infections in Adult Intensive Care UnitsDocument12 pagesThe Efficacy of Daily Chlorhexidine Bathing For Preventing Healthcare-Associated Infections in Adult Intensive Care UnitsKanameMizumiNo ratings yet
- 10) Blood Culture Contaminants - S.dawsonDocument10 pages10) Blood Culture Contaminants - S.dawsonimaguestuserNo ratings yet
- The Effectiveness of Chlorhexidine Bathing in The Prevention of ClabsisDocument9 pagesThe Effectiveness of Chlorhexidine Bathing in The Prevention of Clabsisapi-576596429No ratings yet
- Cui - 2020 - Effects - of - Blood - Flow - On - The - Antibacterial.16Document7 pagesCui - 2020 - Effects - of - Blood - Flow - On - The - Antibacterial.16DodoNo ratings yet
- Tri Bler 2017Document10 pagesTri Bler 2017Thitapus DokbuaNo ratings yet
- Picot Paper Summative FinalDocument10 pagesPicot Paper Summative Finalapi-291122174No ratings yet
- 1 Integrative Review of LiteratureDocument19 pages1 Integrative Review of Literatureapi-531458194No ratings yet
- Nitrogen and Treatment Practice: Paint in The GeneralDocument3 pagesNitrogen and Treatment Practice: Paint in The GeneralMostafa HasanzadehNo ratings yet
- Positive Effect of Care Bundles On Patients With Central Venous Catheter Insertions at A Tertiary Hospital in Beijing, ChinaDocument10 pagesPositive Effect of Care Bundles On Patients With Central Venous Catheter Insertions at A Tertiary Hospital in Beijing, ChinaElfina NataliaNo ratings yet
- Application of The PDCA Cycle For Standardized Nursing Management in Sepsis BundlesBMC AnesthesiologyDocument8 pagesApplication of The PDCA Cycle For Standardized Nursing Management in Sepsis BundlesBMC AnesthesiologyErwin Chicana SoplaNo ratings yet
- Daneman 2020 A Pilot RCT of 7 Vs 14 Days Antibiotic For Bloodstream InfectionDocument11 pagesDaneman 2020 A Pilot RCT of 7 Vs 14 Days Antibiotic For Bloodstream InfectionSelyvira SelyviraNo ratings yet
- Chlorhexidine Bathing and Microbial Contamination in Patients' Bath BasinsDocument7 pagesChlorhexidine Bathing and Microbial Contamination in Patients' Bath BasinsKanameMizumiNo ratings yet
- Inappropriateness in Laboratory Medicine An Elephant in The RoomDocument4 pagesInappropriateness in Laboratory Medicine An Elephant in The RoomomaromranNo ratings yet
- Central LIne Sepsis PresentationDocument11 pagesCentral LIne Sepsis PresentationumeshNo ratings yet
- American Journal of Infection ControlDocument8 pagesAmerican Journal of Infection ControlRizky AdipratamaNo ratings yet
- Colistin Monotherapy Versus Combination Therapy For Carbapenem-Resistant Organisms NEJM EvidenceDocument27 pagesColistin Monotherapy Versus Combination Therapy For Carbapenem-Resistant Organisms NEJM Evidencerac.oncologyNo ratings yet
- Central LIne Sepsis PresentationDocument11 pagesCentral LIne Sepsis PresentationumeshNo ratings yet
- Elevating The Standard of Endoscope Processing Terminal Sterilization of Duodenoscopes Using A Hydrogenperoxide Ozone SterilizerDocument8 pagesElevating The Standard of Endoscope Processing Terminal Sterilization of Duodenoscopes Using A Hydrogenperoxide Ozone SterilizerMicro SoftNo ratings yet
- Impact of Oral Hygiene Involving Toothbrushing Versus Chlorhexidine in The Prevention of Ventilator-Associated Pneumonia A Randomized StudyDocument9 pagesImpact of Oral Hygiene Involving Toothbrushing Versus Chlorhexidine in The Prevention of Ventilator-Associated Pneumonia A Randomized StudyAlessandra Rocha PedrozaNo ratings yet
- 2017-Water During FastingDocument8 pages2017-Water During Fastingpedro vargasNo ratings yet
- Preventing VAPDocument8 pagesPreventing VAPyankesNo ratings yet
- Journal Bedah Ke 2 ShenaDocument12 pagesJournal Bedah Ke 2 Shenasusi susilawatiNo ratings yet
- Deshpande2018 PDFDocument5 pagesDeshpande2018 PDFSixth Batch PharmacyNo ratings yet
- Apt 15802Document16 pagesApt 15802Hadi KuriryNo ratings yet
- JMQ 37 405Document8 pagesJMQ 37 405Software InvestigaciónNo ratings yet
- NAv y No Asociada SHEA 2022Document27 pagesNAv y No Asociada SHEA 2022link0105No ratings yet
- 10 1097@PCC 0000000000000728Document7 pages10 1097@PCC 0000000000000728MarthaAngélicaApNo ratings yet
- Chitosan Nanoparticles PHD ThesisDocument6 pagesChitosan Nanoparticles PHD Thesisfjgmmmew100% (2)
- Dancer 2004Document6 pagesDancer 2004Geby diazNo ratings yet
- ReprocessingendoscopesDocument10 pagesReprocessingendoscopesClara MedinaNo ratings yet
- 2018 Article 1006Document9 pages2018 Article 1006Daniel PuertasNo ratings yet
- 1471 2334 11 278Document6 pages1471 2334 11 278Dwi WirastomoNo ratings yet
- Comparison of Five Commonly Used Automated Susceptibility Testing Methods For Accuracy in The China Antimicrobial Resistance Surveillance System (CARSS) Hospitals PDFDocument12 pagesComparison of Five Commonly Used Automated Susceptibility Testing Methods For Accuracy in The China Antimicrobial Resistance Surveillance System (CARSS) Hospitals PDFntnquynhproNo ratings yet
- Bowel Prep CPG 2019Document6 pagesBowel Prep CPG 2019Ogbonnaya IfeanyichukwuNo ratings yet
- LactobaciloDocument4 pagesLactobaciloHaziel CorroNo ratings yet
- Alcoholic Povidone-Iodine or Chlorhexidine-Based Antiseptic For The Prevention of Central Venous Catheter-Related Infections: In-Use ComparisonDocument8 pagesAlcoholic Povidone-Iodine or Chlorhexidine-Based Antiseptic For The Prevention of Central Venous Catheter-Related Infections: In-Use ComparisonNobita CutterNo ratings yet
- VAP Diagnosis 2009Document8 pagesVAP Diagnosis 2009Illham Setiawan SulistioNo ratings yet
- Vap 2Document8 pagesVap 2ahsan mohammedNo ratings yet
- CHG To Ssi PDFDocument7 pagesCHG To Ssi PDFDian RahmawatiNo ratings yet
- Reducing The Risk of Surgical Site Infections: Does Chlorhexidine Gluconate Provide A Risk Reduction Benefit? PDFDocument7 pagesReducing The Risk of Surgical Site Infections: Does Chlorhexidine Gluconate Provide A Risk Reduction Benefit? PDFBarbara Sakura RiawanNo ratings yet
- 1 s2.0 S2589537023000573 MainDocument11 pages1 s2.0 S2589537023000573 MainSadia MacavilcaNo ratings yet
- Infection Control Procedures in Dialysis - 671.fullDocument3 pagesInfection Control Procedures in Dialysis - 671.fullridha afzalNo ratings yet
- Eria 5Document6 pagesEria 5ruth angelinaNo ratings yet
- Azzam 2011Document2 pagesAzzam 2011Fatma ElzaytNo ratings yet
- Mitigating Isolation Study 2021.12.23.21268326v1.fullDocument10 pagesMitigating Isolation Study 2021.12.23.21268326v1.fullmart0830No ratings yet
- 0300060514561135Document14 pages0300060514561135ardyatri kairaviniNo ratings yet
- The Revolution of Lateral Flow Assay in the Field of AMRDetectionDocument26 pagesThe Revolution of Lateral Flow Assay in the Field of AMRDetectionalbertNo ratings yet
- Clinical Microbiology and Infection: Denise J. Wooding, Horacio BachDocument11 pagesClinical Microbiology and Infection: Denise J. Wooding, Horacio BachendaNo ratings yet
- Environment International: A B A A B D A A A C A BDocument9 pagesEnvironment International: A B A A B D A A A C A Bduverney.gaviriaNo ratings yet
- Ventilator Associated Pneumonia 1Document14 pagesVentilator Associated Pneumonia 1Jennifer ThieleNo ratings yet
- Infection KontrolDocument48 pagesInfection Kontrolrini purwantiNo ratings yet
- Use of a Shared Canister Protocol for the Delivery of Metereddose Inhalers in Mechanically Ventilated Subjects 2016 American Association for Respiratory CareDocument8 pagesUse of a Shared Canister Protocol for the Delivery of Metereddose Inhalers in Mechanically Ventilated Subjects 2016 American Association for Respiratory CareevyNo ratings yet
- Follow-Up Study To Assess The Use and Performance of Household Filters in ZambiaDocument5 pagesFollow-Up Study To Assess The Use and Performance of Household Filters in ZambiaTamara StrattonNo ratings yet
- Parenteral Products: The Preparation and Quality Control of Products for InjectionFrom EverandParenteral Products: The Preparation and Quality Control of Products for InjectionNo ratings yet
- Final Research PaperDocument9 pagesFinal Research Paperapi-444947174No ratings yet
- Clinical Analisis of Sputum Gram StainsDocument7 pagesClinical Analisis of Sputum Gram Stainspelcastre r.No ratings yet
- Clinical Nutrition: Micha Ł Ławinski, Krystyna Majewska, Łukasz Gradowski, Iwona Fo Łtyn, Pierre SingerDocument5 pagesClinical Nutrition: Micha Ł Ławinski, Krystyna Majewska, Łukasz Gradowski, Iwona Fo Łtyn, Pierre SingerBby AdelinaNo ratings yet
- Journal of Hospital Infection: Antiseptic Caps Protect Stopcocks From Internal Bacterial ContaminationDocument3 pagesJournal of Hospital Infection: Antiseptic Caps Protect Stopcocks From Internal Bacterial ContaminationEndhy KurniawanNo ratings yet
- Accreditation For Microbiological LaboratoriesDocument62 pagesAccreditation For Microbiological LaboratoriesFernando CruzNo ratings yet
- Notas Epidemiologicas CDCDocument6 pagesNotas Epidemiologicas CDCClara MedinaNo ratings yet
- NIHR Sheffield Clinical Research Facility: Cleaning and Disinfection of The Sample Processing AreaDocument3 pagesNIHR Sheffield Clinical Research Facility: Cleaning and Disinfection of The Sample Processing AreaTanvir SiddikiNo ratings yet
- Clasen NaDCC2Document9 pagesClasen NaDCC2Farah Fauziah RachmawatieNo ratings yet
- Cleaning Disinfection SterilizationDocument37 pagesCleaning Disinfection SterilizationProfile Info100% (1)
- Global Guidelines For The Prevention of Surgical Site InfectionDocument186 pagesGlobal Guidelines For The Prevention of Surgical Site InfectionLe Ngoc Quynh GiaoNo ratings yet
- Best Practices Environmental Cleaning 2012Document183 pagesBest Practices Environmental Cleaning 2012Clara MedinaNo ratings yet
- Clinical LaboratoriesDocument69 pagesClinical LaboratoriesClara MedinaNo ratings yet
- Multi-Society Guideline For Reprocessing Flexible Gastrointestinal EndoscopesDocument6 pagesMulti-Society Guideline For Reprocessing Flexible Gastrointestinal EndoscopesClara MedinaNo ratings yet
- APIC 2018 DS Antiseptic Update Final R2 6.11.2018Document18 pagesAPIC 2018 DS Antiseptic Update Final R2 6.11.2018Clara MedinaNo ratings yet
- ReprocessingendoscopesDocument10 pagesReprocessingendoscopesClara MedinaNo ratings yet
- Best Practices Environmental Cleaning 2012Document183 pagesBest Practices Environmental Cleaning 2012Clara MedinaNo ratings yet
- CLORHEXIDINE GLUCONATE - S. AureusDocument9 pagesCLORHEXIDINE GLUCONATE - S. AureusClara MedinaNo ratings yet
- Skin-Prep-Best-Practice-Guidance-final-version OKDocument4 pagesSkin-Prep-Best-Practice-Guidance-final-version OKClara MedinaNo ratings yet
- Aagbi Safety Guideline: Skin Antisepsis For Central Neuraxial BlockadeDocument16 pagesAagbi Safety Guideline: Skin Antisepsis For Central Neuraxial BlockadeUNS KAMERA BELAKANGNo ratings yet
- CHLORHEXIDINEDocument48 pagesCHLORHEXIDINEwheiinhyNo ratings yet
- Chlorhexidine Shower Safdar MakiDocument7 pagesChlorhexidine Shower Safdar MakirovypratamaNo ratings yet
- APIC 2018 DS Antiseptic Update Final R2 6.11.2018Document18 pagesAPIC 2018 DS Antiseptic Update Final R2 6.11.2018Clara MedinaNo ratings yet
- All ProblemsDocument107 pagesAll ProblemsjoshiabhijeetNo ratings yet
- 1,16Document138 pages1,16niztgirlNo ratings yet
- CS401 Mcqs For Final TermDocument20 pagesCS401 Mcqs For Final Termsara.arshad.ch4No ratings yet
- Review of oxidative stress and antioxidants in dentistryDocument4 pagesReview of oxidative stress and antioxidants in dentistrySeeptianMaulanaNo ratings yet
- Mischel2004 - Toward An Integrative Science of The PersonDocument24 pagesMischel2004 - Toward An Integrative Science of The PersonTibor GalacziNo ratings yet
- Gujarat Technological University: W.E.F. AY 2018-19Document4 pagesGujarat Technological University: W.E.F. AY 2018-19Premal PatelNo ratings yet
- Ase Utra Military and Law Enforcement ProductsDocument12 pagesAse Utra Military and Law Enforcement ProductsjamesfletcherNo ratings yet
- Book Review - Water, Ecosystems and Society A Confluence of Disciplines. by Jayanta BandyopadhyayDocument2 pagesBook Review - Water, Ecosystems and Society A Confluence of Disciplines. by Jayanta BandyopadhyayPDNo ratings yet
- Troubleshooting Directory for LHB Type RMPU EOG AC CoachesDocument44 pagesTroubleshooting Directory for LHB Type RMPU EOG AC Coachesdivisional electrical engg100% (6)
- Modul 1 - Pengantar Remote SensingDocument60 pagesModul 1 - Pengantar Remote SensingNgurah Ade KalyanaNo ratings yet
- Air Pollution Sources & EffectsDocument2 pagesAir Pollution Sources & EffectsJoanne Ash MajdaNo ratings yet
- Wall Mountable Switches - Wall Mounting GuideDocument3 pagesWall Mountable Switches - Wall Mounting GuideMarcos FilipeNo ratings yet
- Manual stack emission monitoring standardDocument29 pagesManual stack emission monitoring standardsantisal11No ratings yet
- Remote Sensing Mineral Exploration LithiumDocument16 pagesRemote Sensing Mineral Exploration LithiumGerald Darshan MogiNo ratings yet
- Environmental Accounting in The Philippines: by Romulo A. Virola, Sylvia M. de Perio and Eduardo T. AngelesDocument27 pagesEnvironmental Accounting in The Philippines: by Romulo A. Virola, Sylvia M. de Perio and Eduardo T. AngelesLaraNo ratings yet
- Introduction To Coal Handling PlantDocument12 pagesIntroduction To Coal Handling PlantPramod R BidveNo ratings yet
- On K-Distance Degree Index of TreesDocument5 pagesOn K-Distance Degree Index of TreesVelumani sNo ratings yet
- Hospitality Case StudiesDocument26 pagesHospitality Case StudiesKarthik PalaniswamyNo ratings yet
- Chapter 2 - Coordinate GeometryDocument73 pagesChapter 2 - Coordinate GeometryFILIP CEZARNo ratings yet
- Rift Vally BC N RegularDocument308 pagesRift Vally BC N RegularCabdisacid yasinNo ratings yet
- PWR Bi2Document11 pagesPWR Bi2GOMTINo ratings yet
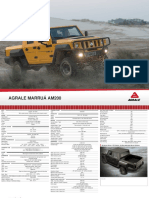
- Off Road and Military Vehicles Off Road Vehicles Agrale Marruaam200 1Document2 pagesOff Road and Military Vehicles Off Road Vehicles Agrale Marruaam200 1Victor SilvaNo ratings yet
- Towards Sustainable Water Management in SoharDocument48 pagesTowards Sustainable Water Management in SoharMiss Preyashi kumarNo ratings yet
- SAE International StandardsAS5553 and AS5553A Counterfeit Electronic Parts Avoidance, Detection, Mitigation and Dispositio PDFDocument35 pagesSAE International StandardsAS5553 and AS5553A Counterfeit Electronic Parts Avoidance, Detection, Mitigation and Dispositio PDFAlejandroAcuñaMaureira100% (1)
- Fe412farm Module N Cost BenefitDocument34 pagesFe412farm Module N Cost BenefitYaswanth NaikNo ratings yet
- Facts on Timber Engineering and StructuresDocument73 pagesFacts on Timber Engineering and StructuresNaresworo NugrohoNo ratings yet
- The Mini Percutaneous Nephrolithotomy (Mini-PCNL) and Percutaneous Nephrolithotomy (PCNL) in Pediatric PatientsDocument4 pagesThe Mini Percutaneous Nephrolithotomy (Mini-PCNL) and Percutaneous Nephrolithotomy (PCNL) in Pediatric PatientsMarius DanilaNo ratings yet
- Algebra II PreAP SimplificationDocument4 pagesAlgebra II PreAP SimplificationSummer SharmaNo ratings yet
- Population Density: Factors and Global DistributionDocument16 pagesPopulation Density: Factors and Global DistributionRYANJUSTIN NICOLASNo ratings yet
- Pacemaker 180508042454Document86 pagesPacemaker 180508042454padmaNo ratings yet