You might also like
- Format of CertificatesDocument12 pagesFormat of CertificatesrowdysinghNo ratings yet
- Child Admission FormDocument6 pagesChild Admission FormA.N.M. neyaz MorshedNo ratings yet
- HMO Application - DependentDocument1 pageHMO Application - DependentBeybey100% (1)
- Scale Aircraft Modelling December 2017 PDFDocument96 pagesScale Aircraft Modelling December 2017 PDFAnonymous N13Jdn100% (2)
- Valuation in The Airline Industry Excel FileDocument12 pagesValuation in The Airline Industry Excel FilevivekNo ratings yet
- Gender and FamilyDocument21 pagesGender and Familychristian garciaNo ratings yet
- Election Commission ProjectDocument15 pagesElection Commission ProjectYashasiviNo ratings yet
- Microeconomic Theory Basic Principles and Extensions WalterDocument16 pagesMicroeconomic Theory Basic Principles and Extensions WalterMilkerValdezGutierrez100% (1)
- Family Declaration FormDocument1 pageFamily Declaration FormJeyakumara Vel CNo ratings yet
- CGHS FormDocument3 pagesCGHS FormHarpreet SinghNo ratings yet
- Alliance Application Form - DXB & NEDocument2 pagesAlliance Application Form - DXB & NEAnkita NiravNo ratings yet
- 3.2.2 Informed ConsentDocument2 pages3.2.2 Informed ConsentobelkesdinkessukabumiNo ratings yet
- Application For Cghs CardDocument3 pagesApplication For Cghs CardManpreetNo ratings yet
- Is Ha Home School ApplicationDocument8 pagesIs Ha Home School ApplicationSri Hari CharanNo ratings yet
- Melbourne Polytechnic App FormDocument5 pagesMelbourne Polytechnic App FormssshalNo ratings yet
- CGHS Application For Pensioners Autonomous BodiesDocument3 pagesCGHS Application For Pensioners Autonomous BodiesBinu PkNo ratings yet
- Child Admission FormDocument6 pagesChild Admission FormANDREW OGALNo ratings yet
- Ngcdf-Bursary Bomet Central 2Document4 pagesNgcdf-Bursary Bomet Central 2Kenny KingNo ratings yet
- Checklist For Counselling 1Document8 pagesChecklist For Counselling 1Akash KrNo ratings yet
- First GraduateDocument3 pagesFirst GraduateKrishnarajan GNo ratings yet
- Admissio N Form-2011: For Mbbs/Bds in Medical/Dental Colleges of RajasthanDocument11 pagesAdmissio N Form-2011: For Mbbs/Bds in Medical/Dental Colleges of RajasthanJitendra ChoudharyNo ratings yet
- Rte Form I 2016 2017 2Document6 pagesRte Form I 2016 2017 2BasavarajBusnurNo ratings yet
- First GraduateDocument4 pagesFirst GraduateBala MuruganNo ratings yet
- Bursary FormDocument2 pagesBursary FormMuji GillNo ratings yet
- Joining Report 15-16finalDocument10 pagesJoining Report 15-16finalPradeep KumarNo ratings yet
- General Circular For MD October, 2022Document18 pagesGeneral Circular For MD October, 2022akhilNo ratings yet
- Declaration FormDocument1 pageDeclaration Formharpal_abhNo ratings yet
- Format-I Bhagyalaxmi Scheme Application For Enrollment: R.C. Office / N.I.C. Office, BelgaumDocument6 pagesFormat-I Bhagyalaxmi Scheme Application For Enrollment: R.C. Office / N.I.C. Office, BelgaumSumithra MNo ratings yet
- 1.5 Star Learners Centre Registration Form Vmar 2023Document4 pages1.5 Star Learners Centre Registration Form Vmar 2023Brandon TanNo ratings yet
- This Certificate Should Be Produced By: Parent NameDocument3 pagesThis Certificate Should Be Produced By: Parent Namesankarsuper83No ratings yet
- Indus Bank Relative DeclarationDocument2 pagesIndus Bank Relative Declarationnitish_vermasNo ratings yet
- Registration & Consent FormDocument2 pagesRegistration & Consent FormSteve HaighNo ratings yet
- Application For Enrolment: Form No. - 1 National Cadet Corps Senior Division/ Wing Enrolment Form (See Rule 7 and 11)Document4 pagesApplication For Enrolment: Form No. - 1 National Cadet Corps Senior Division/ Wing Enrolment Form (See Rule 7 and 11)Sean May0% (1)
- NGCDF Bursary Form Kipkelion West 2022 2023Document3 pagesNGCDF Bursary Form Kipkelion West 2022 2023Hsea KipngetichNo ratings yet
- Nutkins Registration Pack 2015Document7 pagesNutkins Registration Pack 2015api-287286585No ratings yet
- Agra DH JhegbcddDocument20 pagesAgra DH JhegbcddPrdptiwariNo ratings yet
- Bursary Application Form 2014-2015Document7 pagesBursary Application Form 2014-2015inyasiNo ratings yet
- Enrollment FormDocument7 pagesEnrollment FormDivyesh SharmaNo ratings yet
- Junior Division Enrolment FormDocument8 pagesJunior Division Enrolment FormKailash Joshi100% (1)
- Format of Child Study Report (CSR) : I. General InformationDocument3 pagesFormat of Child Study Report (CSR) : I. General InformationJeen DpiNo ratings yet
- Annex 1 To 6Document8 pagesAnnex 1 To 6keshav porwalNo ratings yet
- Application Form IiiDocument6 pagesApplication Form IiibajomumbaseNo ratings yet
- GMC RamagundamDocument8 pagesGMC Ramagundamnooreenshaheri77No ratings yet
- Parental Consent Medical FormDocument2 pagesParental Consent Medical FormRonnie Valladores Jr.No ratings yet
- Application Form For Cghs CardDocument3 pagesApplication Form For Cghs CardHarik CNo ratings yet
- Beneficiary Consular CasesDocument3 pagesBeneficiary Consular CasesHasmen AndalNo ratings yet
- Substance Drug Abuseand Alcoholismfor Students AnnexuresDocument2 pagesSubstance Drug Abuseand Alcoholismfor Students AnnexuresVENELSSEN JOHNS CLASS VINo ratings yet
- Sec Bursary Application Form 2024Document2 pagesSec Bursary Application Form 2024ismashkuruiNo ratings yet
- Application Form For Compassionate AppointmentsDocument4 pagesApplication Form For Compassionate AppointmentsRavi Shankar JoshiNo ratings yet
- Application Form For Compassionate AppointmentsDocument4 pagesApplication Form For Compassionate AppointmentsMallela JyothiNo ratings yet
- Registration Form: P. O. Box 30443 - 00100, NAIROBI, KENYA Website: Email: Folio No: ..........................Document4 pagesRegistration Form: P. O. Box 30443 - 00100, NAIROBI, KENYA Website: Email: Folio No: ..........................Muthoni Wa GachieNo ratings yet
- Joining Final - EducompDocument12 pagesJoining Final - EducompBibind VasuNo ratings yet
- Ipmt FormDocument5 pagesIpmt FormTarinder SinghNo ratings yet
- NCC 2022-23Document5 pagesNCC 2022-23lbspgcollege mgsNo ratings yet
- Annexure - A: Name & Signature of The Student Name & Signature of The Parent/GuardianDocument4 pagesAnnexure - A: Name & Signature of The Student Name & Signature of The Parent/GuardiankumarsaurabhvidyaNo ratings yet
- Affidavit by Parent - StudentDocument2 pagesAffidavit by Parent - Student43045731No ratings yet
- Exchange Form ScholarshipDocument2 pagesExchange Form ScholarshipAna Simina MihaiNo ratings yet
- Surat Akuan Sumpah - Declare Refugee 5Document1 pageSurat Akuan Sumpah - Declare Refugee 5EDMUND CHEONGNo ratings yet
- Revised Declaration FormDocument1 pageRevised Declaration FormThamizh VaananNo ratings yet
- Reletive Declaration yDocument1 pageReletive Declaration ydipakshawbazaarmoneyNo ratings yet
- The National Health Insurance Management Authority: Application For Registration As A MemberDocument3 pagesThe National Health Insurance Management Authority: Application For Registration As A MemberRichard シNo ratings yet
- Application For Registration FormDocument5 pagesApplication For Registration FormarielNo ratings yet
- Provisional Answer KeyDocument11 pagesProvisional Answer KeyFreshflowerNo ratings yet
- O Selim Candidate PackDocument8 pagesO Selim Candidate PackOmar SelimNo ratings yet
- A.M. 1693 The Reformed GentlemanDocument93 pagesA.M. 1693 The Reformed GentlemanMitchell JohnsonNo ratings yet
- Respondent 2007 - Asia Cup MootDocument31 pagesRespondent 2007 - Asia Cup MootNabilBariNo ratings yet
- Unit 2 Second PortfolioDocument3 pagesUnit 2 Second PortfolioSimran PannuNo ratings yet
- Journeyto India by Joni Patry BWDocument7 pagesJourneyto India by Joni Patry BWVigneshwaran MuruganNo ratings yet
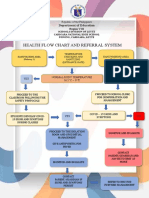
- Health Flow Chart and Referral System: Department of EducationDocument2 pagesHealth Flow Chart and Referral System: Department of EducationWendy TablaNo ratings yet
- A.C. No. 10537 - Ramirez vs. Atty. MargalloDocument6 pagesA.C. No. 10537 - Ramirez vs. Atty. MargalloDennis Jay A. ParasNo ratings yet
- Schweppes Egypt - Premiumization: Marketplace Performance AwardsDocument10 pagesSchweppes Egypt - Premiumization: Marketplace Performance AwardsAdam AbdelkhalikiNo ratings yet
- Flashcards Word PictureDocument34 pagesFlashcards Word PictureNur Lisa Ahmad ZakiNo ratings yet
- Gayatris and Other Mantras For AssistanceDocument42 pagesGayatris and Other Mantras For AssistanceBalrajGoulikarNo ratings yet
- Adr-Group 7Document33 pagesAdr-Group 7Charl DayritNo ratings yet
- Tranning Letter FormatDocument9 pagesTranning Letter FormatVivekNo ratings yet
- HUPERETASDocument1 pageHUPERETASKhalied NoynayNo ratings yet
- After BrexitDocument7 pagesAfter Brexityosmeilys.ramirezNo ratings yet
- JB APUSH Unit 1 Topic 1.6Document9 pagesJB APUSH Unit 1 Topic 1.6Graham NicholsNo ratings yet
- Law and It AssignmentDocument16 pagesLaw and It AssignmentQadir JavedNo ratings yet
- The Workshop of The Sculptor Thutmose inDocument14 pagesThe Workshop of The Sculptor Thutmose inYara LinariNo ratings yet
- Sources PageDocument4 pagesSources Pageapi-106353803No ratings yet
- Professional Practice Law and Ethics 1st Unit Lecture NotesDocument27 pagesProfessional Practice Law and Ethics 1st Unit Lecture NotesRammohanreddy RajidiNo ratings yet
- Unit 15 (Final) PDFDocument12 pagesUnit 15 (Final) PDFआई सी एस इंस्टीट्यूटNo ratings yet
- instaPDF - in Kargil War Heroes Saheed List With Photo 301Document6 pagesinstaPDF - in Kargil War Heroes Saheed List With Photo 301uruuva phenixNo ratings yet
- Fixed Assets: User GuideDocument165 pagesFixed Assets: User GuideAi Li HengNo ratings yet
- District Memo On Deped Ed Run For Students Wave 2 - EditedDocument4 pagesDistrict Memo On Deped Ed Run For Students Wave 2 - EditedNioganElemNo ratings yet
- Introduction To ERP SystemDocument2 pagesIntroduction To ERP SystemLeann BathanNo ratings yet