You might also like
- Lapsus Multitrauma - Id.enDocument73 pagesLapsus Multitrauma - Id.enTantyaNo ratings yet
- Chapter 11 - The Appendicular Skeletal SystemDocument6 pagesChapter 11 - The Appendicular Skeletal Systemmedianoche191% (11)
- OMM Fellows ReviewDocument178 pagesOMM Fellows ReviewTony Ziherl100% (1)
- Buikstra and Ubelaker 1994 Standard Cap 7 PDFDocument23 pagesBuikstra and Ubelaker 1994 Standard Cap 7 PDFDan Reese100% (3)
- Orthopedic: Lec.11 DR - Hasan Abdulhadi.MDocument10 pagesOrthopedic: Lec.11 DR - Hasan Abdulhadi.MninaNo ratings yet
- Pelvic InjuriesDocument35 pagesPelvic InjuriesJavier Saad100% (1)
- 76040138-Referat-Fraktur-Pelvis EditDocument34 pages76040138-Referat-Fraktur-Pelvis Editsri wulanNo ratings yet
- Pelvic Fractures - These Can Kill YouDocument20 pagesPelvic Fractures - These Can Kill YouSurgicalgownNo ratings yet
- AsuasuasususuDocument67 pagesAsuasuasususuAnonymous 7dsX2F8nNo ratings yet
- Fracture of Pelvis: Basaria Manurung, DRG Pembimbing: Dr. Dicky Mulyadi, DR., SP - OT (K)Document28 pagesFracture of Pelvis: Basaria Manurung, DRG Pembimbing: Dr. Dicky Mulyadi, DR., SP - OT (K)basaria manurungNo ratings yet
- Pelvicinjuries 181026150723Document106 pagesPelvicinjuries 181026150723EntesipatyNo ratings yet
- Pelvic Fracture: Supervisor: MR JeffDocument22 pagesPelvic Fracture: Supervisor: MR JeffTitusNo ratings yet
- Open Book FractureDocument31 pagesOpen Book FractureMUHAMMAD ADLI ADNAN BIN JAMIL STUDENTNo ratings yet
- Pelvis and HipDocument90 pagesPelvis and Hipalsead798No ratings yet
- Clavicle FractureDocument33 pagesClavicle FractureNitin AggarwalNo ratings yet
- Fraktur ClaviculaDocument23 pagesFraktur ClaviculaayuradityoNo ratings yet
- Pelvictrauma 151103203943 Lva1 App6892Document40 pagesPelvictrauma 151103203943 Lva1 App6892Navin BalajiNo ratings yet
- LBM 4 Step 1 1. ATLS Protocol Step 2 1. How Is The Biomechanic of Trauma? 2. How Is The Anatomical Structure of Hip and Leg?Document6 pagesLBM 4 Step 1 1. ATLS Protocol Step 2 1. How Is The Biomechanic of Trauma? 2. How Is The Anatomical Structure of Hip and Leg?indahsariNo ratings yet
- Shoulder Trauma Fractures and Dislocations-Orthoinfo - AaosDocument6 pagesShoulder Trauma Fractures and Dislocations-Orthoinfo - Aaosapi-228773845No ratings yet
- Pelvic Trauma: Stud.: Andris Džeriņš, MF V 5.gr. Mentor: Dr. Med. Ruta JakušonokaDocument46 pagesPelvic Trauma: Stud.: Andris Džeriņš, MF V 5.gr. Mentor: Dr. Med. Ruta JakušonokaRendy SusantoNo ratings yet
- Pelvic Injury (Autosaved)Document44 pagesPelvic Injury (Autosaved)abhishek chaudharyNo ratings yet
- Pelvic Injruies 2Document57 pagesPelvic Injruies 2King salehNo ratings yet
- Лекция № 12 англDocument31 pagesЛекция № 12 англchai rinNo ratings yet
- Pelvic TraumaDocument20 pagesPelvic Traumachehak.kumar2000No ratings yet
- ClaviculaDocument24 pagesClaviculaoktavia indahNo ratings yet
- Evaluation and Management of Acute Cervical Spine Trauma-RKY-finalDocument84 pagesEvaluation and Management of Acute Cervical Spine Trauma-RKY-finalRickky MDNo ratings yet
- Pelvic Injruies 1Document43 pagesPelvic Injruies 1King salehNo ratings yet
- دكتور ايوب OrthopaedicDocument14 pagesدكتور ايوب OrthopaedicDrAyyoub AbboodNo ratings yet
- Pelvic FracturesDocument32 pagesPelvic FracturesAgeng BudianantiNo ratings yet
- Fracture-Dislocation of The Hip-KaizarDocument69 pagesFracture-Dislocation of The Hip-KaizarKaizar Ennis100% (1)
- Foot Calcaneal Fracture - Rehabilitation ProtocolDocument7 pagesFoot Calcaneal Fracture - Rehabilitation ProtocolAdmirNo ratings yet
- REFERAT Lumbar Compression FractureDocument25 pagesREFERAT Lumbar Compression FractureTaufik Ghockil ZlaluwNo ratings yet
- Hip Condition PhysiopediaDocument96 pagesHip Condition PhysiopediaPrethy PhilipNo ratings yet
- Pelvic FractureDocument89 pagesPelvic FractureAndreas RendraNo ratings yet
- Pelvic FractureDocument31 pagesPelvic Fracturepoe3No ratings yet
- Clavicle AO Surgery Reference (2023)Document399 pagesClavicle AO Surgery Reference (2023)Wael GabrNo ratings yet
- Dislocations: Diagnosis, Management, and Complications: Marvin H. Meyers, M.D.Document12 pagesDislocations: Diagnosis, Management, and Complications: Marvin H. Meyers, M.D.Unoscientris StupaNo ratings yet
- William C. Cottrell, MD AbstractDocument4 pagesWilliam C. Cottrell, MD AbstractmalaNo ratings yet
- Pelvis: Stable Pelvic FracturesDocument4 pagesPelvis: Stable Pelvic FracturesEloise PateñoNo ratings yet
- Shoulder Sports InjuryDocument12 pagesShoulder Sports InjuryfriskaNo ratings yet
- Anterior Cruciate Ligament Tear DefinitionDocument8 pagesAnterior Cruciate Ligament Tear DefinitionEunice IquinaNo ratings yet
- Pelvic Ring InjuryDocument124 pagesPelvic Ring InjuryPicha PichiNo ratings yet
- I. Dr. Yoyos - Unstable Pelvic Fracture Jam 14Document42 pagesI. Dr. Yoyos - Unstable Pelvic Fracture Jam 14Rsud Malinau Ppk BludNo ratings yet
- Pelvic Fractures PksDocument48 pagesPelvic Fractures PksprinceveettoorNo ratings yet
- Hip Fractures-Orthoinfo - AaosDocument9 pagesHip Fractures-Orthoinfo - Aaosapi-228773845No ratings yet
- Pelvic Trauma: Continuing Education ActivityDocument13 pagesPelvic Trauma: Continuing Education ActivityEdu Ayala RivadeneiraNo ratings yet
- SPINEDocument2 pagesSPINEKhyathi SriNo ratings yet
- Gadline PrsentationDocument12 pagesGadline PrsentationsumardiNo ratings yet
- Seminar On Upper Limb FractureDocument166 pagesSeminar On Upper Limb FractureArko dutta100% (1)
- Diagnostic Imaging - 9 - Regional Pathologies and Evaluation - Cervical and Lumbar RegionDocument41 pagesDiagnostic Imaging - 9 - Regional Pathologies and Evaluation - Cervical and Lumbar RegionAly MssreNo ratings yet
- Rotator CuffDocument46 pagesRotator CuffLiza Perez- Pagatpatan100% (2)
- Traumas of Spine and Pelvis. Done By:moldir Akynbay 17-40-01Document25 pagesTraumas of Spine and Pelvis. Done By:moldir Akynbay 17-40-01Moldir AkynbayNo ratings yet
- Acetabular FracturesDocument69 pagesAcetabular Fracturesmohammad farhanNo ratings yet
- Fraktur VertebraeDocument41 pagesFraktur VertebraeTomy WiknaNo ratings yet
- Dislokasi Panggul & BahuDocument42 pagesDislokasi Panggul & BahuAnton TrihartantoNo ratings yet
- C14 - Coloana Vertebrala Engleza 2Document109 pagesC14 - Coloana Vertebrala Engleza 2Andreea DanielaNo ratings yet
- Materi Kuliah FK ULM 2022 - Lower Extremity I - Hip & KneeDocument61 pagesMateri Kuliah FK ULM 2022 - Lower Extremity I - Hip & Kneezaki ridhoniNo ratings yet
- Fracture FemurDocument28 pagesFracture FemurKulsoom ShahNo ratings yet
- Pelvic TraumaDocument11 pagesPelvic TraumaБека ЭзугбаяNo ratings yet
- Acetabulum Set 5 P 81Document25 pagesAcetabulum Set 5 P 81Mukunth IyerNo ratings yet
- Urethral InjuriesDocument41 pagesUrethral InjuriesTahleel Altaf100% (1)
- Fractures of Clavicle AserDocument44 pagesFractures of Clavicle AserHeba ElgoharyNo ratings yet
- Internal Derangements of KneeDocument92 pagesInternal Derangements of KneeAzad Roxo100% (3)
- Bladder Injury: Types, Mechanisms, and Diagnostic Imaging: Jordan S. Gross, MD Scott Rotenberg, MD Mindy M. Horrow, MDDocument38 pagesBladder Injury: Types, Mechanisms, and Diagnostic Imaging: Jordan S. Gross, MD Scott Rotenberg, MD Mindy M. Horrow, MDTantyaNo ratings yet
- Mononucleosis Mono Kissing Disease Epstein-Barr Virus (EBV) Toxoplasmosis 1Document3 pagesMononucleosis Mono Kissing Disease Epstein-Barr Virus (EBV) Toxoplasmosis 1TantyaNo ratings yet
- Strategies For Periodontal Risk Assessment and PrognosisDocument12 pagesStrategies For Periodontal Risk Assessment and PrognosisTantyaNo ratings yet
- Dysfunction of The Sacroiliac Joint and Its Treatment : Richard L. Dontigny, BS, PTTDocument14 pagesDysfunction of The Sacroiliac Joint and Its Treatment : Richard L. Dontigny, BS, PTTSandroLaoNo ratings yet
- Lec 3 &4 (Skeletal Appendicular Skeleton)Document123 pagesLec 3 &4 (Skeletal Appendicular Skeleton)Nengah VindiNo ratings yet
- A&p - All Files in One PDFDocument201 pagesA&p - All Files in One PDFandreeaNo ratings yet
- Leson Plan FEMALE PELVISDocument8 pagesLeson Plan FEMALE PELVISPreeti SawantNo ratings yet
- First Periodical Test Science & Health IvDocument4 pagesFirst Periodical Test Science & Health Ivcrisanto_oroceoNo ratings yet
- WWW Slideshare Net SurajDhara2 Forensic Medicine Mcqs PDFDocument19 pagesWWW Slideshare Net SurajDhara2 Forensic Medicine Mcqs PDFShrutiNo ratings yet
- TEMA 5 InglesDocument9 pagesTEMA 5 InglesrebecasanchobarNo ratings yet
- Lectured By: Dr. Jesus J. Gracilla Transcribed By: Beverly YuDocument7 pagesLectured By: Dr. Jesus J. Gracilla Transcribed By: Beverly YuFamela Anne GOmez MadambaNo ratings yet
- Bruzek 2002 AJPADocument12 pagesBruzek 2002 AJPAthereeseNo ratings yet
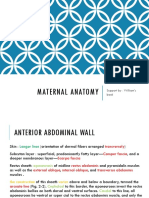
- Chapter 2 Maternal Anatomy WilliamsDocument60 pagesChapter 2 Maternal Anatomy WilliamsDiskaAstariniNo ratings yet
- Handbook of Orthopaedic TraumatologyDocument145 pagesHandbook of Orthopaedic TraumatologyDonna Williams100% (2)
- Table of Joints in Lower LimbDocument5 pagesTable of Joints in Lower LimbVijay Pradeep100% (3)
- Final Obstetrics and GynacologyDocument88 pagesFinal Obstetrics and Gynacologysis8100% (2)
- Exclusive Ospe Notebook 1 1Document50 pagesExclusive Ospe Notebook 1 1Naeem Al HasanNo ratings yet
- Randolph Stone - Polarity Therapy - Collected Works Vol IIDocument232 pagesRandolph Stone - Polarity Therapy - Collected Works Vol IIFelipe Prado100% (1)
- Surface AnatomyDocument63 pagesSurface AnatomyCodie SimoneauxNo ratings yet
- The Birth Process - StudentDocument327 pagesThe Birth Process - StudentMio RuikoNo ratings yet
- Sahar Nahar RaiDocument17 pagesSahar Nahar RaiAd AstraNo ratings yet
- Lower Extremity TraumaDocument72 pagesLower Extremity TraumaMariamNo ratings yet
- 5 6289750532911268052 PDFDocument472 pages5 6289750532911268052 PDFvasanthrslv100% (6)
- Clinical Anatomy of The Vulva, Vagina, Lower Pelvis, and PerineumDocument20 pagesClinical Anatomy of The Vulva, Vagina, Lower Pelvis, and PerineumJacobMsangNo ratings yet
- Appendicular SkeletonDocument27 pagesAppendicular SkeletonSheena SapaoNo ratings yet
- Surgical Female Urogenital Anatomy - UpToDateDocument57 pagesSurgical Female Urogenital Anatomy - UpToDateErickNo ratings yet
- 06 Bones of Lower LimbDocument42 pages06 Bones of Lower LimbbnvjNo ratings yet
- "That Which Was Missing": The Archaeology of Castration by Kathryn ReuschDocument45 pages"That Which Was Missing": The Archaeology of Castration by Kathryn ReuschAlmaas NaveedNo ratings yet
- BonesDocument25 pagesBonesJohnvee Magana100% (2)
- Ultrasound in Obstretics PDFDocument40 pagesUltrasound in Obstretics PDFcarcobe3436100% (1)