You might also like
- Personality Assessment TestsDocument5 pagesPersonality Assessment TestsDennis KimNo ratings yet
- Mind and Emotions: A Universal Treatment For Emotional DisordersDocument9 pagesMind and Emotions: A Universal Treatment For Emotional DisordersNew Harbinger Publications100% (7)
- Sach Sentence Completion Test InterpretationDocument4 pagesSach Sentence Completion Test Interpretationrupal arora67% (3)
- Admit OrdersDocument2 pagesAdmit OrdersTariq Niaz Ahmad, MDNo ratings yet
- Male Female PsychologyDocument38 pagesMale Female PsychologyParamjit SharmaNo ratings yet
- SBAR Change of Shift Report: DoctorDocument2 pagesSBAR Change of Shift Report: DoctorLora100% (1)
- WHO Lab Quality Management SystemDocument246 pagesWHO Lab Quality Management SystemMigori Art100% (1)
- Nueva Ecija University of Science and TechnologyDocument3 pagesNueva Ecija University of Science and TechnologyRay Anne GonzalesNo ratings yet
- Code Blue Form: Part of The Medical RecordDocument1 pageCode Blue Form: Part of The Medical RecordRimky Mps0% (1)
- Medsurg Report SheetDocument1 pageMedsurg Report Sheetjjuplifter100% (3)
- Fundamentals of Nursing Transes 3Document4 pagesFundamentals of Nursing Transes 3Louise TorresNo ratings yet
- Cinical Note Sheet: Prsenting ComplaintsDocument2 pagesCinical Note Sheet: Prsenting ComplaintsDhananjay SainiNo ratings yet
- Code Blue Form: Part of The Medical RecordDocument1 pageCode Blue Form: Part of The Medical RecordassepNo ratings yet
- Nursing Brain - JGDocument2 pagesNursing Brain - JGapi-280874783No ratings yet
- دليل الوصف الوظيفي للعاملين بالمستشفياتDocument210 pagesدليل الوصف الوظيفي للعاملين بالمستشفياتmax00ha100% (4)
- Ob Clinical Worksheet - IntrapartumDocument8 pagesOb Clinical Worksheet - Intrapartumcandice lavigneNo ratings yet
- QualifiedPhysio MSK Interview Preparation Pack PDFDocument48 pagesQualifiedPhysio MSK Interview Preparation Pack PDFUkpabi GinikachiNo ratings yet
- Organizational WorksheetDocument4 pagesOrganizational WorksheetJennifer AprilNo ratings yet
- Technical Requirements in Vitro Diagnostics (IVD)Document4 pagesTechnical Requirements in Vitro Diagnostics (IVD)Raydoon Sadeq100% (1)
- Night BeforeDocument3 pagesNight BeforeChris MoffettNo ratings yet
- DigitalDiagnost C50 CSV2 High Performance - 0.1 - TXT - TypicalDocument23 pagesDigitalDiagnost C50 CSV2 High Performance - 0.1 - TXT - Typicalemilio paredesNo ratings yet
- HIV Related Policies and Guidelines Issuances: Training On HIV Counseling and Testing and Facility-Based HIV ScreeningDocument77 pagesHIV Related Policies and Guidelines Issuances: Training On HIV Counseling and Testing and Facility-Based HIV ScreeningJovania B.No ratings yet
- K9 TECC Casualty Card FINAL PDFDocument2 pagesK9 TECC Casualty Card FINAL PDFariel4dariel4larutaNo ratings yet
- Borang HemodialisisDocument2 pagesBorang HemodialisisMahayun Raneh0% (1)
- Uttar PradeshDocument7 pagesUttar PradeshPawani Gupta100% (1)
- Sim Scenario 4Document31 pagesSim Scenario 4lilchibaby3161No ratings yet
- Fever Clerking Sheet KKBSPDocument2 pagesFever Clerking Sheet KKBSPEd ThomasNo ratings yet
- Telemetry Recognition WorkbookDocument29 pagesTelemetry Recognition WorkbookQueenNo ratings yet
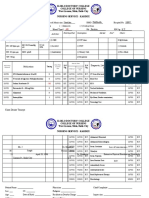
- Iloilo Doctors' College College of Nursing West Avenue, Molo, Iloilo City Nursing Service - KardexDocument4 pagesIloilo Doctors' College College of Nursing West Avenue, Molo, Iloilo City Nursing Service - KardexKiara Denise TamayoNo ratings yet
- Nursing Care Plan Example NR450Document8 pagesNursing Care Plan Example NR450J15No ratings yet
- NCP - Impaired Gas Exchange (COPD)Document3 pagesNCP - Impaired Gas Exchange (COPD)Karen Joy ItoNo ratings yet
- Forms Med WardDocument11 pagesForms Med WardDell GarciaNo ratings yet
- 12ni. Non-Invasive Ventilation (BiPAP) For COPD (University Hospital of South Manchester, Dec 2011)Document7 pages12ni. Non-Invasive Ventilation (BiPAP) For COPD (University Hospital of South Manchester, Dec 2011)ManuNo ratings yet
- WakeMed Non-Hemorrhagic Stroke-TIA Admission Orders Rev 12-07iDocument3 pagesWakeMed Non-Hemorrhagic Stroke-TIA Admission Orders Rev 12-07iNafilah SyellaNo ratings yet
- Kardex - Acute PancreatitisDocument5 pagesKardex - Acute PancreatitisKiara Denise TamayoNo ratings yet
- Total Hip and Knee ReplacementsDocument57 pagesTotal Hip and Knee ReplacementsBryndenNo ratings yet
- Nurse Brain SheetsDocument1 pageNurse Brain SheetsBryan NguyenNo ratings yet
- Cookeville Regional Medical Center Severe Sepsis/Septic Shock Clinical PathwayDocument4 pagesCookeville Regional Medical Center Severe Sepsis/Septic Shock Clinical PathwayArnelli HutagalungNo ratings yet
- Endotracheal Intubation Flow SheetDocument2 pagesEndotracheal Intubation Flow SheetsafasayedNo ratings yet
- DkaordersDocument1 pageDkaordersTaufiqurrokhman RofiiNo ratings yet
- Adult Outpatient Chemotherapy Order Form: Abvd Q28DaysDocument1 pageAdult Outpatient Chemotherapy Order Form: Abvd Q28DaysJOHN LOPERANo ratings yet
- ICU General Admission Orders: OthersDocument2 pagesICU General Admission Orders: OthersHANIMNo ratings yet
- General Surgery Admission Order Set - Sample Template: Code StatusDocument4 pagesGeneral Surgery Admission Order Set - Sample Template: Code StatusEricka SwordNo ratings yet
- Flow SheetDocument1 pageFlow Sheetcolin_powersNo ratings yet
- Vicpostoporderform WebDocument2 pagesVicpostoporderform WebJunaid ShahNo ratings yet
- INP Bedside WorksheetDocument2 pagesINP Bedside WorksheetHarrison RigorNo ratings yet
- MTPTTP ED ProformaDocument3 pagesMTPTTP ED ProformaRajin MaahiNo ratings yet
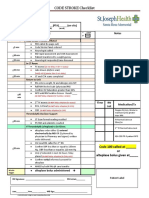
- CODE STROKE Checklist:: NotesDocument1 pageCODE STROKE Checklist:: NotesAdam MochtarNo ratings yet
- k9 Tecc Casualty Card FinalDocument2 pagesk9 Tecc Casualty Card Finalariel4dariel4laruta100% (1)
- KMC Audit Jan 2023Document3 pagesKMC Audit Jan 2023group4clmmrhNo ratings yet
- Kardex - Traumatic Spine InjuryDocument5 pagesKardex - Traumatic Spine InjuryKiara Denise TamayoNo ratings yet
- Code Blue Form: Part of The Medical RecordDocument1 pageCode Blue Form: Part of The Medical RecordPrio Si IyoNo ratings yet
- Anaesthesia Notes Sudan PDFDocument1 pageAnaesthesia Notes Sudan PDFihtisham1No ratings yet
- PT PTT INR Na CL BUN K Ca Creat HGB WBC PlateletsDocument1 pagePT PTT INR Na CL BUN K Ca Creat HGB WBC PlateletsRyan Drake RomeroNo ratings yet
- 107.premedical FormatDocument2 pages107.premedical FormatKrish KrishNo ratings yet
- Implementation Nursing Orders / Approaches RationaleDocument2 pagesImplementation Nursing Orders / Approaches RationaleAngelique Jade EnriquezNo ratings yet
- ENDORSEMENT FORM Converted MergedDocument2 pagesENDORSEMENT FORM Converted MergedrjNo ratings yet
- LSU/Ochsner Ophthalmology Residency Program: Surgical Case FormDocument2 pagesLSU/Ochsner Ophthalmology Residency Program: Surgical Case FormShaun IttiaraNo ratings yet
- PGDT Protocol Summary ReferenceDocument32 pagesPGDT Protocol Summary Referenceghg sddNo ratings yet
- Aminoglycoside & Vancomycin: Basic TDMDocument57 pagesAminoglycoside & Vancomycin: Basic TDMft84nzzc92No ratings yet
- Learner'S Worksheet: Clinical RotationDocument3 pagesLearner'S Worksheet: Clinical RotationLecery Sophia WongNo ratings yet
- Acute Decompensated Heart Failure Topic Discussion HandoutDocument4 pagesAcute Decompensated Heart Failure Topic Discussion Handoutapi-641524095No ratings yet
- Myocardial Infarct Checklist: TIMELINE // DateDocument2 pagesMyocardial Infarct Checklist: TIMELINE // DateMohd Syamirulah RahimNo ratings yet
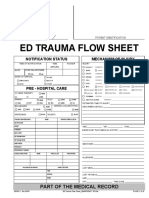
- Ed Trauma Flow Sheet: Part of The Medical RecordDocument6 pagesEd Trauma Flow Sheet: Part of The Medical RecordsafasayedNo ratings yet
- ALS Practical Assessment Tool 2018Document5 pagesALS Practical Assessment Tool 2018MorganeNo ratings yet
- Kardex - End Stage Renal FailureDocument5 pagesKardex - End Stage Renal FailureKiara Denise TamayoNo ratings yet
- NorthernDocument12 pagesNorthernAprilian Ayu SitaNo ratings yet
- Csu, Stanislaus B.S.N. Clinical Plan of Care Patient DataDocument18 pagesCsu, Stanislaus B.S.N. Clinical Plan of Care Patient Dataapi-284664489No ratings yet
- LSU/Ochsner Ophthalmology Residency Program: Surgical Case FormDocument2 pagesLSU/Ochsner Ophthalmology Residency Program: Surgical Case FormShaun IttiaraNo ratings yet
- BAENA, Nicole - Monitoring SheetDocument2 pagesBAENA, Nicole - Monitoring SheetnicoletbaenaNo ratings yet
- Flow Sheet TemplateDocument4 pagesFlow Sheet TemplateIulia Tania AndronacheNo ratings yet
- refeeding $ &ftt د مني رشادDocument5 pagesrefeeding $ &ftt د مني رشادReda ZizoNo ratings yet
- Topic 1 What Is Patient Safety?: (Concepts and Prospects)Document21 pagesTopic 1 What Is Patient Safety?: (Concepts and Prospects)Reda ZizoNo ratings yet
- Topic 1 What Is Patient Safety?: (Concepts and Prospects)Document21 pagesTopic 1 What Is Patient Safety?: (Concepts and Prospects)Reda ZizoNo ratings yet
- Strategic Planning As An Approach of Improving The Human Resources Performance in The Algerian Public Hospitals: Case StudyDocument18 pagesStrategic Planning As An Approach of Improving The Human Resources Performance in The Algerian Public Hospitals: Case StudyReda ZizoNo ratings yet
- Acute Division - Beds Available: (National Standards For Safer Better Healthcare)Document153 pagesAcute Division - Beds Available: (National Standards For Safer Better Healthcare)Reda ZizoNo ratings yet
- Developing and Planning Strategies of Health Services in Jenin City in The Light of The Citys Physical DevelopmentDocument244 pagesDeveloping and Planning Strategies of Health Services in Jenin City in The Light of The Citys Physical DevelopmentReda ZizoNo ratings yet
- Red Cross CPR Guidelines PDFDocument31 pagesRed Cross CPR Guidelines PDFandrewh3No ratings yet
- Sabarimala: Virtual-Q Booking CouponDocument2 pagesSabarimala: Virtual-Q Booking CouponHarinath Hari0% (1)
- Name: Date: - Year/Section:: Task 1: PAR-Q and YOU Questionnaire (Prior To The Activity Test)Document3 pagesName: Date: - Year/Section:: Task 1: PAR-Q and YOU Questionnaire (Prior To The Activity Test)Angela Louise Smiths0% (1)
- Informative Speech TextDocument2 pagesInformative Speech TextadzwinjNo ratings yet
- Chinese Contractor Wins Kuwait Remediation WorkDocument4 pagesChinese Contractor Wins Kuwait Remediation WorkSanabel EliasNo ratings yet
- FKG Catalogue 2015Document68 pagesFKG Catalogue 2015Septimiu TiplicaNo ratings yet
- Mining Legislation and Mineral Development in ZambiaDocument35 pagesMining Legislation and Mineral Development in ZambiaNathan MwewaNo ratings yet
- Reaction Paper (Group4)Document3 pagesReaction Paper (Group4)MARC MARVIN PALOMARESNo ratings yet
- Sacred Ash (3.5e Epic Spell) - D&D WikiDocument1 pageSacred Ash (3.5e Epic Spell) - D&D WikiJuan MonsalveNo ratings yet
- STAT 2300 Test 1 Review - S19Document19 pagesSTAT 2300 Test 1 Review - S19teenwolf4006No ratings yet
- Ew MeritDocument120 pagesEw MeritShlok RathodNo ratings yet
- Emotional Body Pain Chart: How It WorksDocument3 pagesEmotional Body Pain Chart: How It Worksdaniel50% (2)
- Tork Catalogue UkiDocument102 pagesTork Catalogue UkiBirdsNo ratings yet
- The Problem and Background of The StudyDocument6 pagesThe Problem and Background of The StudyAileen ElegadoNo ratings yet
- PrelimDocument3 pagesPrelimJM RebancosNo ratings yet
- RRL 2Document4 pagesRRL 2MURILLO, FRANK JOMARI C.No ratings yet
- Roleplay ISBAR Bhs InggrisDocument2 pagesRoleplay ISBAR Bhs InggrisPutri fajrianti SultanNo ratings yet
- ResearchDocument70 pagesResearchMagud, Jemverick Jan Leonard O.No ratings yet
- NHS Dental Statistics For England 2018-19, Annual Report (PAS) - NHS DigitalDocument3 pagesNHS Dental Statistics For England 2018-19, Annual Report (PAS) - NHS DigitalRowayda NourNo ratings yet
- J Clinic Periodontology - 2018 - Caton - A New Classification Scheme For Periodontal and Peri Implant Diseases andDocument8 pagesJ Clinic Periodontology - 2018 - Caton - A New Classification Scheme For Periodontal and Peri Implant Diseases andVõ Thị Mỹ NhungNo ratings yet