You might also like
- LIGHT Pulmo Ventilation Sleep Apnea DR ConstantinoDocument6 pagesLIGHT Pulmo Ventilation Sleep Apnea DR ConstantinoMiguel Cuevas DolotNo ratings yet
- Hypo and HyperventilationDocument5 pagesHypo and Hyperventilationkristian markus delos santosNo ratings yet
- Central Regulation of RespirationDocument54 pagesCentral Regulation of RespirationsamNo ratings yet
- Respiration and EmotionFrom EverandRespiration and EmotionY. HarukiNo ratings yet
- Respiration: Control of Ventilation: Learning ObjectivesDocument4 pagesRespiration: Control of Ventilation: Learning Objectiveshuldani-1No ratings yet
- Cecilia, Issaiah Nicolle-Pneumothorax-NcpDocument7 pagesCecilia, Issaiah Nicolle-Pneumothorax-NcpIssaiah Nicolle Cecilia100% (1)
- Shams - P28 - Control of Breathing (1h)Document17 pagesShams - P28 - Control of Breathing (1h)UmerNo ratings yet
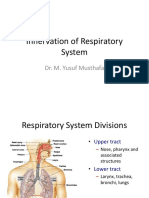
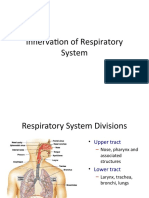
- Innervation of Respiratory SystemDocument21 pagesInnervation of Respiratory SystemYusuf MusthafaNo ratings yet
- 4.control of VentilationDocument40 pages4.control of VentilationEbin EbenezerNo ratings yet
- Respirasi ControlDocument50 pagesRespirasi Controlrinaldy IX9No ratings yet
- Trastornos de Sueño-ResíracionDocument18 pagesTrastornos de Sueño-ResíracionDra Carolina Escalante Neurologa de AdultosNo ratings yet
- Control of Ventilation: Lectures On Respiratory PhysiologyDocument52 pagesControl of Ventilation: Lectures On Respiratory PhysiologyNagib HadianNo ratings yet
- Innervation of Respiratory SystemDocument21 pagesInnervation of Respiratory SystemYusuf MusthafaNo ratings yet
- NCM 112 LEC Topic 2 Oxygenation Current Health History Physical Examination Normal Abnormal Breath Sounds Breathing PatternsDocument7 pagesNCM 112 LEC Topic 2 Oxygenation Current Health History Physical Examination Normal Abnormal Breath Sounds Breathing PatternsViviene Faye FombuenaNo ratings yet
- Organization of The Respiratory Control System 2007Document53 pagesOrganization of The Respiratory Control System 2007Vincent VicuñaNo ratings yet
- Anaphylactic Shock ReaderDocument3 pagesAnaphylactic Shock ReaderzipheleleNo ratings yet
- Physiological Overview in Relation To PracticeDocument52 pagesPhysiological Overview in Relation To PracticedrkhaledassemNo ratings yet
- Respiration - Imp Topics-1Document14 pagesRespiration - Imp Topics-1SHAHSINANo ratings yet
- NCP Ineffective Breathing ActualDocument3 pagesNCP Ineffective Breathing ActualArian May Marcos100% (1)
- MEDSRUG Respiratory System NotesDocument6 pagesMEDSRUG Respiratory System NotesMichaela Katrice MacabangunNo ratings yet
- Respiratory Disorders and Sleep 2008, Vol.3, Issues 4Document120 pagesRespiratory Disorders and Sleep 2008, Vol.3, Issues 4Karolina RamirezNo ratings yet
- Pengaturan Sistem RespirasiDocument18 pagesPengaturan Sistem RespirasiMaulidya MagfirahNo ratings yet
- Anestesia y Analgesia BSAVA-319-341Document23 pagesAnestesia y Analgesia BSAVA-319-341angel.mendozaNo ratings yet
- C3C4 Quiz 2Document25 pagesC3C4 Quiz 2Mariel AbatayoNo ratings yet
- Asincronia 2022Document8 pagesAsincronia 2022EN BUNo ratings yet
- NCP Ineffective Breathing PatternDocument3 pagesNCP Ineffective Breathing PatternMiar QuestNo ratings yet
- RespirationDocument10 pagesRespirationADWAIT LALUNo ratings yet
- Respi DisordersDocument19 pagesRespi DisordersAzielle Joyce RosquetaNo ratings yet
- Ineffective Airway Clearance Related To BronchospasmDocument2 pagesIneffective Airway Clearance Related To BronchospasmReylan Garcia100% (4)
- RespDocument23 pagesRespAyessa D. RosalitaNo ratings yet
- General Anaesthetics PharmacologyDocument87 pagesGeneral Anaesthetics Pharmacologysultan khanNo ratings yet
- Pi Is 0960982216310557Document2 pagesPi Is 0960982216310557Ridski D. MiruNo ratings yet
- NCP - ANAPHYLACTIC SHOCK..2pdfDocument6 pagesNCP - ANAPHYLACTIC SHOCK..2pdfLycah RotoneNo ratings yet
- NCM 112 N LECTURE MidtermDocument42 pagesNCM 112 N LECTURE MidtermVivien IgnacioNo ratings yet
- Sleepandbreathing: Kelly Newton,, Vipin Malik,, Teofilo Lee-ChiongDocument6 pagesSleepandbreathing: Kelly Newton,, Vipin Malik,, Teofilo Lee-ChiongVijay KumarNo ratings yet
- Clinical Teaching On Ventilator Settings and ModeDocument21 pagesClinical Teaching On Ventilator Settings and Modejyoti punia100% (1)
- Slow Deep BreathingDocument17 pagesSlow Deep BreathingpluigiaNo ratings yet
- Nelson Textbook of Pediatrics (2-Volume Set) by Robert M. Kliegman, Bonita F. Stanton, Joseph W. ST Geme III, Nina F. SchorDocument312 pagesNelson Textbook of Pediatrics (2-Volume Set) by Robert M. Kliegman, Bonita F. Stanton, Joseph W. ST Geme III, Nina F. SchorFaisal MomenNo ratings yet
- NCP For Scenario BreathingDocument4 pagesNCP For Scenario Breathingmy moznNo ratings yet
- Mbbscbmeph-1 No023525Document40 pagesMbbscbmeph-1 No023525Aritro RoyNo ratings yet
- (06!03!05) - Lower Brainstem Functions (Compatibility Mode) - 1ppDocument21 pages(06!03!05) - Lower Brainstem Functions (Compatibility Mode) - 1ppjNo ratings yet
- A Case Study of Bronchial Asthma in Acute Exacerbation (Baiae)Document10 pagesA Case Study of Bronchial Asthma in Acute Exacerbation (Baiae)Janina RojoNo ratings yet
- Pola PernafasanDocument3 pagesPola PernafasanSeto Wahyu PrasetyoNo ratings yet
- A Modern Approach To Cough ManagementDocument4 pagesA Modern Approach To Cough ManagementSorin PalcuNo ratings yet
- Probing The Psychophysiology of The Airways: Physical Activity, Experienced Emotion, and Facially Expressed EmotionDocument13 pagesProbing The Psychophysiology of The Airways: Physical Activity, Experienced Emotion, and Facially Expressed EmotionAlexo JaimezNo ratings yet
- Ikhlas Muhammad Jenie Physiology Department: Fkik UmyDocument56 pagesIkhlas Muhammad Jenie Physiology Department: Fkik Umyade ayuningsih utamiNo ratings yet
- Inhaled AnestheticsDocument13 pagesInhaled AnestheticsCzar SyNo ratings yet
- Name: L.J.A AGE: 20 Years Old SEX: Male CC: Cough and DOB Admitting/Working Diagnosis: AsthmaDocument2 pagesName: L.J.A AGE: 20 Years Old SEX: Male CC: Cough and DOB Admitting/Working Diagnosis: AsthmaMae Therese B. MAGNONo ratings yet
- NCP Ineffective BreathingDocument6 pagesNCP Ineffective BreathingCuttie Anne GalangNo ratings yet
- DR Zainuri - Otot PernapasanDocument37 pagesDR Zainuri - Otot PernapasanAdhiatma DotNo ratings yet
- Topic 7 Resp SystDocument11 pagesTopic 7 Resp SystFamilia Macovei Haralambie-AndreeaNo ratings yet
- Respiratory Diseases Chapter From Nelson Textbook of PediatricsDocument312 pagesRespiratory Diseases Chapter From Nelson Textbook of PediatricsMilan Andrejevic100% (1)
- Regulation of RespirationDocument46 pagesRegulation of Respirationnirilib89% (9)
- Bronchospasm During Anaesthesia Update 2011Document5 pagesBronchospasm During Anaesthesia Update 2011Vanessa HermioneNo ratings yet
- General Anesthetics TRANSDocument15 pagesGeneral Anesthetics TRANSNikki Tuazon BartolomeNo ratings yet
- Asma KabulllllDocument30 pagesAsma KabulllllChoirul WizaNo ratings yet
- Control of RespirationDocument13 pagesControl of RespirationArunchandar VelusamyNo ratings yet
- Chapter 8 - Clinical Examination of The ElbowDocument3 pagesChapter 8 - Clinical Examination of The ElbowkenthepaNo ratings yet
- Appeal Letter FfsDocument1 pageAppeal Letter FfsAndrea LaBarberaNo ratings yet
- Effectiveness of The Motor Relearning ApproachDocument5 pagesEffectiveness of The Motor Relearning ApproachZahid MehmoodNo ratings yet
- Managment of Sepsis and Septic ShockDocument2 pagesManagment of Sepsis and Septic ShockDavid Simon CruzNo ratings yet
- Allergies: A Protective Mechanism Out of ControlDocument29 pagesAllergies: A Protective Mechanism Out of Controlडा. सत्यदेव त्यागी आर्यNo ratings yet
- Data Pending Rs Citra Arafiq 25112018Document20 pagesData Pending Rs Citra Arafiq 25112018Zahirman HamzahNo ratings yet
- PRO Post Natal AssessmentDocument9 pagesPRO Post Natal AssessmentMali KanuNo ratings yet
- Band Keratopathy ArticleDocument9 pagesBand Keratopathy ArticleDecha Pradea MaulinaNo ratings yet
- 2464 8451 1 PBDocument6 pages2464 8451 1 PBSuwenda MadeNo ratings yet
- Persepsi Mahasiswi Tentang Kanker Payudara Dan Perilakunya Terhadap Pencegahan Kanker Payudara Di Fakultas Keperawatan Universitas AndalasDocument8 pagesPersepsi Mahasiswi Tentang Kanker Payudara Dan Perilakunya Terhadap Pencegahan Kanker Payudara Di Fakultas Keperawatan Universitas AndalasAfifah AzhariNo ratings yet
- All About Iris Tumors Dr. Schefler1 PDFDocument2 pagesAll About Iris Tumors Dr. Schefler1 PDFTruly GracevaNo ratings yet
- Annexure A6-8 A4Document15 pagesAnnexure A6-8 A4bathinsreenivasNo ratings yet
- Maturity Onset Diabetes of The Young: Clinical Characteristics, Diagnosis and ManagementDocument10 pagesMaturity Onset Diabetes of The Young: Clinical Characteristics, Diagnosis and ManagementatikahanifahNo ratings yet
- Hepatitis in Children (Hep A, B, C)Document26 pagesHepatitis in Children (Hep A, B, C)sarNo ratings yet
- 5-Article Text-53-1-10-20210513Document5 pages5-Article Text-53-1-10-20210513yuliana bayuNo ratings yet
- ARTG Summary For Health NavigatorDocument2 pagesARTG Summary For Health NavigatorinergetixNo ratings yet
- Episode ListDocument25 pagesEpisode ListhectorNo ratings yet
- CHO Special MCQs #1Document7 pagesCHO Special MCQs #1Praveen LaxkarNo ratings yet
- Interaksi Obat Dengan Nutrisi EnteralDocument5 pagesInteraksi Obat Dengan Nutrisi EnteralRijantono Franciscus MariaNo ratings yet
- A Study of Cisplatin Chemoteraphy and Hearing LossDocument4 pagesA Study of Cisplatin Chemoteraphy and Hearing LossPriska AmeliaNo ratings yet
- PediatricsDocument33 pagesPediatricsnageshwarioshNo ratings yet
- SMP 3510 Heller Chapter34Document48 pagesSMP 3510 Heller Chapter34Ari DewiyantiNo ratings yet
- Reference Books For CSIR-NET - BioTecNikaDocument11 pagesReference Books For CSIR-NET - BioTecNikaDr-Katari VenkateshNo ratings yet
- A Study of PlacentaDocument9 pagesA Study of PlacentaDr. Zain FazalNo ratings yet
- Hirschsprung DiseaseDocument19 pagesHirschsprung DiseaseJudith PurificacionNo ratings yet
- ANATOM 128 Brochure-ReDocument8 pagesANATOM 128 Brochure-ReAli MirzaNo ratings yet
- Article With BhajanDocument4 pagesArticle With BhajanBibek SutradharNo ratings yet
- EO094 COVIDRecommendationsDocument4 pagesEO094 COVIDRecommendationsTMJ4 News50% (2)
- Disinfection & Sterilization 2Document49 pagesDisinfection & Sterilization 2YasminNo ratings yet
- PIIS0015028212007017Document9 pagesPIIS0015028212007017marinaNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (24)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)