You might also like
- Anti Plate Let 2016Document14 pagesAnti Plate Let 2016Desti Ratna PutriNo ratings yet
- NSAIDs, DMARDs, Analgesics & Gout DrugsDocument114 pagesNSAIDs, DMARDs, Analgesics & Gout DrugsMani Jee100% (1)
- Acetylsalicylic Acid (Aspirin) : 1190159 3 GradeDocument8 pagesAcetylsalicylic Acid (Aspirin) : 1190159 3 GradeAbdelrhman AboodaNo ratings yet
- Individual NSAIDs Mechanisms and UsesDocument4 pagesIndividual NSAIDs Mechanisms and UsesJsnanbjrihNo ratings yet
- Guide to NSAIDs (Non-Steroidal Anti-Inflammatory DrugsDocument40 pagesGuide to NSAIDs (Non-Steroidal Anti-Inflammatory DrugsHarini Bala100% (1)
- AAS - Side EffectsDocument10 pagesAAS - Side EffectsTiago SanTanaNo ratings yet
- Australian PrescriberDocument3 pagesAustralian PrescriberMohamed OmerNo ratings yet
- Ecotrin (ASA 81mg)Document3 pagesEcotrin (ASA 81mg)E100% (1)
- NSAIDsDocument54 pagesNSAIDsAlaaNo ratings yet
- DR - Hussam Lec 3 Drugs Affecting Blood 2023 4Document13 pagesDR - Hussam Lec 3 Drugs Affecting Blood 2023 4ManWol JangNo ratings yet
- NSAIDs (Aspirin)Document13 pagesNSAIDs (Aspirin)Muhammad ZamimNo ratings yet
- Anti Pyretic 2013Document15 pagesAnti Pyretic 2013Faizah Al GhamdiNo ratings yet
- Antipyretic-Analgesic and Antiinflammatory DrugsDocument46 pagesAntipyretic-Analgesic and Antiinflammatory DrugsAYU SUKARNI PUTRINo ratings yet
- Myrin P ForteDocument3 pagesMyrin P ForteJohn Zedric Villanueva ArciagaNo ratings yet
- Product Monograph: (Acetylsalicylic Acid Chewable Tablets, USP) 81 MGDocument31 pagesProduct Monograph: (Acetylsalicylic Acid Chewable Tablets, USP) 81 MGعبدالعزيز بدرNo ratings yet
- Aspirin and Salicylates: SourcesDocument3 pagesAspirin and Salicylates: SourcesahmedNo ratings yet
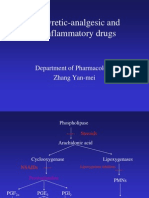
- Antipyretic-Analgesic and Antiinflammatory Drugs: Department of Pharmacology Zhang Yan-MeiDocument39 pagesAntipyretic-Analgesic and Antiinflammatory Drugs: Department of Pharmacology Zhang Yan-MeiIshu SethiNo ratings yet
- Prostaglandins and NSAIDs in InflammationDocument21 pagesProstaglandins and NSAIDs in InflammationAmr SalemNo ratings yet
- Non Steroidal Anti Inflammatory Drugs 72768501 2Document68 pagesNon Steroidal Anti Inflammatory Drugs 72768501 2AnushaNo ratings yet
- Aspilets ECDocument5 pagesAspilets ECJerry SerapionNo ratings yet
- Salicylates: Common Name: Acetylsalicylic Acid IUPAC Name: 2-Acetoxybenzoic Acid Molecular Formula: C H ODocument3 pagesSalicylates: Common Name: Acetylsalicylic Acid IUPAC Name: 2-Acetoxybenzoic Acid Molecular Formula: C H OJaica Mangurali TumulakNo ratings yet
- Discovery of Aspirin: Presented By: Group 5Document42 pagesDiscovery of Aspirin: Presented By: Group 5LimYiNo ratings yet
- Acetylcysteine 200mg (Siran, Reolin)Document5 pagesAcetylcysteine 200mg (Siran, Reolin)ddandan_2No ratings yet
- Drug Study TemplateDocument30 pagesDrug Study Template2230299No ratings yet
- Arcoxia Uses, Dosage, Side EffectsDocument8 pagesArcoxia Uses, Dosage, Side EffectsGeorge FogNo ratings yet
- Product MonographDocument33 pagesProduct Monographعبدالعزيز بدرNo ratings yet
- Lec9 د ذو الفقارDocument4 pagesLec9 د ذو الفقارMohammed JaberNo ratings yet
- Acetazolamide-Acetazolamide Injection, Powder, Lyophilized, For Solution Xgen Pharmaceuticals DJB, IncDocument9 pagesAcetazolamide-Acetazolamide Injection, Powder, Lyophilized, For Solution Xgen Pharmaceuticals DJB, Incandi hasri ainunNo ratings yet
- Summary of Product Characteristics: Adults (Including Elderly Patients)Document8 pagesSummary of Product Characteristics: Adults (Including Elderly Patients)Yuzark GumintangNo ratings yet
- Acetazolamide injection for IV useDocument13 pagesAcetazolamide injection for IV useandi hasri ainunNo ratings yet
- Anti-Inflammatory Drugs Lec 3 and 4 LatestDocument37 pagesAnti-Inflammatory Drugs Lec 3 and 4 Latests.nilormee1201No ratings yet
- ParacetamolDocument78 pagesParacetamolMichalNo ratings yet
- Revised Drug IndexDocument76 pagesRevised Drug IndexMinette SantosNo ratings yet
- Analgesic Antipyretic Antiinflamatory DrugsDocument50 pagesAnalgesic Antipyretic Antiinflamatory DrugsNavneet KhuranaNo ratings yet
- Nsaids Nonsteroidal Anti-Inflammatory Drugs: Maher Khdour Msc. Phd. Clinical PharmacyDocument65 pagesNsaids Nonsteroidal Anti-Inflammatory Drugs: Maher Khdour Msc. Phd. Clinical PharmacyYousef JafarNo ratings yet
- Acetylsalicilic Acid 400mg + Ascorbic Acid 240mg (Aspirin C)Document10 pagesAcetylsalicilic Acid 400mg + Ascorbic Acid 240mg (Aspirin C)asdwasdNo ratings yet
- Antihypertensive Drug InteractionsDocument8 pagesAntihypertensive Drug InteractionsNur AzimahNo ratings yet
- NSAIDs GuideDocument39 pagesNSAIDs GuideSufyan Ashraf100% (1)
- AcetazolamideDocument4 pagesAcetazolamideAnkit RuhilNo ratings yet
- Committee For Veterinary Medicinal ProductsDocument7 pagesCommittee For Veterinary Medicinal Productsvetma1No ratings yet
- Acetazolamide For Injection, USPDocument5 pagesAcetazolamide For Injection, USPbishoy.youssef.cpiNo ratings yet
- C - VVV VV VVVV VVV - VVV VV - VVVV VV VVDocument3 pagesC - VVV VV VVVV VVV - VVV VV - VVVV VV VVBea Angela Bithao AnonoyNo ratings yet
- Salicylates: Elora Apantaku, MDDocument12 pagesSalicylates: Elora Apantaku, MDElora ApantakuNo ratings yet
- Anti Inflamatory Drugs AINSDocument39 pagesAnti Inflamatory Drugs AINSEl FaroukNo ratings yet
- Antigout PDFDocument21 pagesAntigout PDFshaifNo ratings yet
- Non Steroidal Anti Inflammatory DrugsDocument29 pagesNon Steroidal Anti Inflammatory DrugsanelublaNo ratings yet
- Drug StudyDocument6 pagesDrug StudyChickz HunterNo ratings yet
- Quiz 1: General MOADocument38 pagesQuiz 1: General MOASajeda A. HadiNo ratings yet
- TabletsDocument6 pagesTabletsRupesh Kumar DuttaNo ratings yet
- Ace InhibitoriDocument12 pagesAce InhibitoriMedical StudentNo ratings yet
- Antpyretic-Analgesic and Antinlammatory DrugsDocument38 pagesAntpyretic-Analgesic and Antinlammatory DrugskasondaNo ratings yet
- Acetylsalicilic Acid 100mg (Aspirin Cardio, Micropirin, Cartia, Tevapirin, Godamed)Document8 pagesAcetylsalicilic Acid 100mg (Aspirin Cardio, Micropirin, Cartia, Tevapirin, Godamed)asdwasdNo ratings yet
- Brand Name: NoneDocument18 pagesBrand Name: NoneEmeka JusticeNo ratings yet
- Acetazolamide (Uramox)Document5 pagesAcetazolamide (Uramox)ddandan_2No ratings yet
- 3 Analgesic Anitpyretic InfamDocument10 pages3 Analgesic Anitpyretic InfamAnonymous dRAu54No ratings yet
- Antenatal Glucocorticoid Therapy and Fetal Lung MaturationDocument32 pagesAntenatal Glucocorticoid Therapy and Fetal Lung Maturationcclaire197% (37)
- Materi 7 - Gagal Ginjal AkutDocument30 pagesMateri 7 - Gagal Ginjal AkutTegar Muhamad RifkiNo ratings yet
- Mefenamic Acid Indication, Dosage, Side Effect, Precaution MIMS MalaysiaDocument1 pageMefenamic Acid Indication, Dosage, Side Effect, Precaution MIMS MalaysianuruladyanisaifuzzamanNo ratings yet
- Anticoagulation Module 2Document13 pagesAnticoagulation Module 2angelmedurNo ratings yet
- Duke Radiology Contrast Media Guidelines Final 10.13.16 PDFDocument35 pagesDuke Radiology Contrast Media Guidelines Final 10.13.16 PDFAdina BatajuNo ratings yet
- The Star News January 28, 2016Document36 pagesThe Star News January 28, 2016The Star NewsNo ratings yet
- Neurological Physiotherapy Evaluation FormDocument13 pagesNeurological Physiotherapy Evaluation FormShruti100% (10)
- Charity Marathon Risk AssessmentDocument9 pagesCharity Marathon Risk Assessmentamarnadh100% (1)
- Thesis Final Last PDFDocument46 pagesThesis Final Last PDFDeepalNo ratings yet
- (Recent Results in Cancer Research 203) Florian Otto, Manfred P. Lutz (Eds.) - Early Gastrointestinal CancerDocument244 pages(Recent Results in Cancer Research 203) Florian Otto, Manfred P. Lutz (Eds.) - Early Gastrointestinal CancerTolga ŞanlıNo ratings yet
- CRQs For The Final FRCA (Oxford Speciality Training Revision Texts) (Mar 21, 2021) - (0198850301) - (Oxford University Press)Document286 pagesCRQs For The Final FRCA (Oxford Speciality Training Revision Texts) (Mar 21, 2021) - (0198850301) - (Oxford University Press)AE100% (2)
- A Comprehensive Review On Gynura Procumbens Leaves - International Journal of PharmacognosyDocument6 pagesA Comprehensive Review On Gynura Procumbens Leaves - International Journal of PharmacognosyKurniati FadilahNo ratings yet
- Topic English EssayDocument8 pagesTopic English Essayd3gpmvqw100% (2)
- CHCFAM003 Student Assessment Task 1Document19 pagesCHCFAM003 Student Assessment Task 1kishor khatriNo ratings yet
- Chapter 39: Hematologic Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument5 pagesChapter 39: Hematologic Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
- Migmar Tsering (Mike) S ResumeDocument3 pagesMigmar Tsering (Mike) S Resumeapi-284044370No ratings yet
- PATHOPHYSIOLOGYofDocument3 pagesPATHOPHYSIOLOGYofRose Si CheeksNo ratings yet
- AMR Policy Insights November2016 - OECDDocument12 pagesAMR Policy Insights November2016 - OECDtanishtarun06No ratings yet
- Nursing Clinical Self-Directed LearningDocument4 pagesNursing Clinical Self-Directed LearningDyan Bianca Suaso LastimosaNo ratings yet
- Pathology Slides by Organ 1-1Document36 pagesPathology Slides by Organ 1-1Lin AdutNo ratings yet
- Respiratory NotesDocument2 pagesRespiratory NotesLidy CastilloNo ratings yet
- FNCP MaglayaDocument8 pagesFNCP MaglayaVaronNo ratings yet
- Bruce Protocol PST313Document12 pagesBruce Protocol PST313Michael GuzikNo ratings yet
- Family Centered CareDocument7 pagesFamily Centered CareSirisha ChelvaNo ratings yet
- Non-Fermenting and Miscellaneous Gram Negative BacilliDocument33 pagesNon-Fermenting and Miscellaneous Gram Negative BacilliLin Sison Vitug100% (1)
- McEntee, Asst Prof Laurence Lower Back Pain A4 301120 PDFDocument2 pagesMcEntee, Asst Prof Laurence Lower Back Pain A4 301120 PDFRamesh SinghNo ratings yet
- Handbook of Dialysis 5th Edition ReviewDocument1 pageHandbook of Dialysis 5th Edition ReviewSurafel KebedeNo ratings yet
- Walker V Good Shepherd CHRONOLOGYDocument34 pagesWalker V Good Shepherd CHRONOLOGYMiddle CNo ratings yet
- The Role of Diet and Nutrition On Mental Health and WellbeingDocument3 pagesThe Role of Diet and Nutrition On Mental Health and WellbeingMeha RajNo ratings yet
- Rxprep 2019 Study Chart: ST ND RD TH THDocument5 pagesRxprep 2019 Study Chart: ST ND RD TH THYazan100% (2)
- BSU College of Nursing Assessment FormDocument17 pagesBSU College of Nursing Assessment FormLucille Allen100% (32)
- Management For The Drowning PatientDocument27 pagesManagement For The Drowning PatientDanieli Bello Chimer da SilvaNo ratings yet
- Locally Endemic Diseases ControlhandoutDocument3 pagesLocally Endemic Diseases ControlhandoutEshiebel OrganistaNo ratings yet
- Brainsci 11 00924 v3Document15 pagesBrainsci 11 00924 v3Tanvi ManjrekarNo ratings yet