You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Case Study On Jaundice-1Document30 pagesCase Study On Jaundice-1kamini ChoudharyNo ratings yet
- Seminar On deDocument23 pagesSeminar On dekamini ChoudharyNo ratings yet
- Role - of - Curriculum - Coordinator 3Document8 pagesRole - of - Curriculum - Coordinator 3kamini Choudhary100% (1)
- 0 - 01-05-2020 Zoom Classes DetailsDocument9 pages0 - 01-05-2020 Zoom Classes Detailskamini ChoudharyNo ratings yet
- Faculty of Nursing - Zoom Online Classes DetailsDocument9 pagesFaculty of Nursing - Zoom Online Classes Detailskamini ChoudharyNo ratings yet
- Case Presentation On Pharyngitis2Document10 pagesCase Presentation On Pharyngitis2kamini ChoudharyNo ratings yet
- Assignment On Standardized and Non Standardized Tool 2s by Kamini c2Document11 pagesAssignment On Standardized and Non Standardized Tool 2s by Kamini c2kamini ChoudharyNo ratings yet
- Nursing Care Plan On FeverDocument15 pagesNursing Care Plan On Feverkamini ChoudharyNo ratings yet
- Assignment On QuestionnaireDocument8 pagesAssignment On Questionnairekamini ChoudharyNo ratings yet
- Prakash Institute of Nursing Greater NoidaDocument9 pagesPrakash Institute of Nursing Greater Noidakamini ChoudharyNo ratings yet
- Assignment On Pharamcological Aspects - BY KAMINI2Document9 pagesAssignment On Pharamcological Aspects - BY KAMINI2kamini ChoudharyNo ratings yet
- Case Study On Jaundice-1Document30 pagesCase Study On Jaundice-1kamini Choudhary100% (5)
- Case Plan On Diarrhoea (Medical Surgical Nursing)Document15 pagesCase Plan On Diarrhoea (Medical Surgical Nursing)kamini ChoudharyNo ratings yet
- Assignment On Family Welfare-1Document5 pagesAssignment On Family Welfare-1kamini ChoudharyNo ratings yet
- Sub - Medical Surgical Nursing: Assignment On Neurological AssessmentDocument11 pagesSub - Medical Surgical Nursing: Assignment On Neurological Assessmentkamini Choudhary100% (1)
- Scoring by Kamini Chaudhary2Document7 pagesScoring by Kamini Chaudhary2kamini ChoudharyNo ratings yet
- NCP DIarrheaDocument8 pagesNCP DIarrheakamini ChoudharyNo ratings yet
- ASSIGNMENT ON Distance by KaminiDocument9 pagesASSIGNMENT ON Distance by Kaminikamini ChoudharyNo ratings yet
- Health Education by Kamini MSNDocument15 pagesHealth Education by Kamini MSNkamini Choudhary100% (2)
- COLLECTIVE BARGAINING - by Kamini ChaudharyDocument7 pagesCOLLECTIVE BARGAINING - by Kamini Chaudharykamini ChoudharyNo ratings yet
- Assignment On Tools For Data Collection by Kamini23Document6 pagesAssignment On Tools For Data Collection by Kamini23kamini Choudhary100% (1)
- Sub - Medical Surgical Nursing: Assignment On CVP MonitoringDocument11 pagesSub - Medical Surgical Nursing: Assignment On CVP Monitoringkamini ChoudharyNo ratings yet
- Assignment On Curriculum Research by KaminiDocument6 pagesAssignment On Curriculum Research by Kaminikamini ChoudharyNo ratings yet
- Cbe & Obe by KaminiDocument8 pagesCbe & Obe by Kaminikamini Choudhary100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- SCM (Subway Project Report)Document13 pagesSCM (Subway Project Report)Beast aNo ratings yet
- Goldhofer FTV 850 BrochureDocument2 pagesGoldhofer FTV 850 BrochureMauroNo ratings yet
- Elements of Romanticism in The Poetry of W. B. Yeats: Romantic InfluencesDocument8 pagesElements of Romanticism in The Poetry of W. B. Yeats: Romantic InfluencesSadman Shaid SaadNo ratings yet
- Board Replacement CasesDocument41 pagesBoard Replacement CasesNadeeshNo ratings yet
- 1962 Gibson Johnny SmithDocument5 pages1962 Gibson Johnny SmithLuisNo ratings yet
- Nissan Copper LTDDocument11 pagesNissan Copper LTDankit_shahNo ratings yet
- Soldier of Fortune PDFDocument208 pagesSoldier of Fortune PDFNixel SpielNo ratings yet
- 08 Activity 1 (10) (LM)Document2 pages08 Activity 1 (10) (LM)Jhanine Mae Oriola FortintoNo ratings yet
- Awakened Citizen Programme-Report-class VII-2014Document4 pagesAwakened Citizen Programme-Report-class VII-2014bhsgeneral r m saraswathi50% (4)
- Assignment 2 Unit 20 Fully Completed - ReviewedDocument5 pagesAssignment 2 Unit 20 Fully Completed - Reviewedchris.orisawayiNo ratings yet
- Material Specification - 077154C-000-JSS-1700-009 - DDocument13 pagesMaterial Specification - 077154C-000-JSS-1700-009 - DStructures ProductionNo ratings yet
- 5G Transport Slice Control in End-To-End 5G NetworksDocument19 pages5G Transport Slice Control in End-To-End 5G NetworksmorganNo ratings yet
- EN Manual Lenovo Ideapad S130-14igm S130-11igmDocument33 pagesEN Manual Lenovo Ideapad S130-14igm S130-11igmDolgoffNo ratings yet
- Assignment 2 Mat435Document2 pagesAssignment 2 Mat435Arsene LupinNo ratings yet
- AKI in ChildrenDocument43 pagesAKI in ChildrenYonas AwgichewNo ratings yet
- Course Syllabus: Course Code Course Title ECTS CreditsDocument3 pagesCourse Syllabus: Course Code Course Title ECTS CreditsHanaa HamadallahNo ratings yet
- Innerwear Industry Pitch PresentationDocument19 pagesInnerwear Industry Pitch PresentationRupeshKumarNo ratings yet
- MTH100Document3 pagesMTH100Syed Abdul Mussaver ShahNo ratings yet
- Runyankore-Rukiga Dictionary Launch: President Yoweri Museveni's SpeechDocument28 pagesRunyankore-Rukiga Dictionary Launch: President Yoweri Museveni's SpeechThe New Vision50% (2)
- Fighting Techniques of The Early Modern World AD 1500-AD 1763 - Equipment Combat Skills Amp Amp TacticsDocument258 pagesFighting Techniques of The Early Modern World AD 1500-AD 1763 - Equipment Combat Skills Amp Amp Tacticslupoeva100% (3)
- Paediatric Intake Form Modern OT 2018Document6 pagesPaediatric Intake Form Modern OT 2018SefNo ratings yet
- JKJKJDocument3 pagesJKJKJjosecarlosvjNo ratings yet
- 07ercoskun 05 01 PDFDocument23 pages07ercoskun 05 01 PDFjagmadridNo ratings yet
- Parts Catalogue of Foton: (TC2A504-034K)Document132 pagesParts Catalogue of Foton: (TC2A504-034K)МаксимNo ratings yet
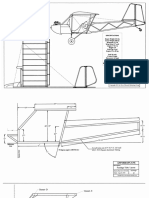
- Plans PDFDocument49 pagesPlans PDFEstevam Gomes de Azevedo85% (34)
- Save Water SpeechDocument4 pagesSave Water SpeechHari Prakash Shukla0% (1)
- Cambridge IGCSE Paper 2Document4 pagesCambridge IGCSE Paper 2irajooo epik zizterNo ratings yet
- Guia de CondensadoresDocument193 pagesGuia de CondensadoresPaola Segura CorreaNo ratings yet
- Release From Destructive Covenants - D. K. OlukoyaDocument178 pagesRelease From Destructive Covenants - D. K. OlukoyaJemima Manzo100% (1)
- 12 Key Principles On Bhava AnalysisDocument28 pages12 Key Principles On Bhava AnalysisDhineshNo ratings yet