
Ethylene Oxide Gas Sterilization of Medical Devices
Ethylene Oxide Gas Sterilization of Medical Devices
You might also like
- PHSS Clarity On GMP Guidance No.3 Qualification of No Touch Transfer For RTU ContainersDocument8 pagesPHSS Clarity On GMP Guidance No.3 Qualification of No Touch Transfer For RTU ContainersAkuWilliamsNo ratings yet
- PHSS Control Strategy White PaperDocument13 pagesPHSS Control Strategy White PaperAkuWilliams100% (1)
- CCS Guide Attachment3 v2Document34 pagesCCS Guide Attachment3 v2elisabetta ghilardi100% (1)
- PDA Journal SeptemberDocument19 pagesPDA Journal SeptemberZia100% (2)
- Smoke Study Article 1Document15 pagesSmoke Study Article 1JAGADISH PHARMACEUTICALSNo ratings yet
- Tim Sandle White Paper EU - GMP - Annex - 1 - The - New - Draft - and - Implications 2020Document15 pagesTim Sandle White Paper EU - GMP - Annex - 1 - The - New - Draft - and - Implications 2020Supriya KapasNo ratings yet
- A Review of Cleanroom Microflora Types, Trends, and Patterns.Document14 pagesA Review of Cleanroom Microflora Types, Trends, and Patterns.Sean NamNo ratings yet
- 41 Sterilization Validation Key Steps To Dose Auditing 1Document2 pages41 Sterilization Validation Key Steps To Dose Auditing 1Vivian CerdasNo ratings yet
- S. No. SOP Title Room No. Responsibility StatusDocument1 pageS. No. SOP Title Room No. Responsibility Statusjpmaurya77No ratings yet
- Astm A668 Tensile ReqDocument1 pageAstm A668 Tensile ReqDilip Gajanan Namjoshi100% (1)
- Kleiberit PUR 501 - FISPQDocument8 pagesKleiberit PUR 501 - FISPQYuri SouzaNo ratings yet
- Use of Chemical & Biological Indicators - 2014 2Document56 pagesUse of Chemical & Biological Indicators - 2014 2jerimiah_manzonNo ratings yet
- PHSS - Clarity - in - GMP - Guidance - Barrier - Isolator - Technology - Leak Integrity Classes - v1Document12 pagesPHSS - Clarity - in - GMP - Guidance - Barrier - Isolator - Technology - Leak Integrity Classes - v1AkuWilliamsNo ratings yet
- ETO Sterilization ValidationDocument44 pagesETO Sterilization ValidationCRYSTAL2100100% (1)
- What Is Disinfectant ValidationDocument4 pagesWhat Is Disinfectant Validationrouss1906No ratings yet
- Multicenter Study On Incubation Conditions For Environmental Monitoring and Aseptic Process SimulationDocument9 pagesMulticenter Study On Incubation Conditions For Environmental Monitoring and Aseptic Process SimulationBLUEPRINT Integrated Engineering ServicesNo ratings yet
- General Chapters - 1222 - Terminally Sterilized Pharmaceutical Products-Parametric ReleaseDocument5 pagesGeneral Chapters - 1222 - Terminally Sterilized Pharmaceutical Products-Parametric ReleaseSuman Katteboina0% (1)
- RedBook BIT MayJune2012Document5 pagesRedBook BIT MayJune2012Liman SetiawanNo ratings yet
- Sanitization of Pharmaceutical FacilitiesDocument14 pagesSanitization of Pharmaceutical FacilitiesTim Sandle100% (1)
- Autoclave Validation: Presented by Paul Yeatman Bsc. MicrobiologistDocument17 pagesAutoclave Validation: Presented by Paul Yeatman Bsc. Microbiologistzfo302No ratings yet
- Cleanroom MicrobiologyDocument14 pagesCleanroom MicrobiologyKraken UrNo ratings yet
- 1231 - Water For Pharmaceutical PurposesDocument29 pages1231 - Water For Pharmaceutical PurposesLinh Nguyen100% (2)
- EO Annual Requalification ReviewDocument30 pagesEO Annual Requalification ReviewVenkatesh VenkateshNo ratings yet
- Guide For Determining The Confidence Interval Using ExcelDocument2 pagesGuide For Determining The Confidence Interval Using ExcelTim Sandle100% (3)
- IVT Network - Biodecontamination of Cleanrooms and Laboratories Using Gassing Systems - 2017-09-20Document13 pagesIVT Network - Biodecontamination of Cleanrooms and Laboratories Using Gassing Systems - 2017-09-20Le KhoaNo ratings yet
- Sterilization Validation QsiteDocument52 pagesSterilization Validation Qsiteskype2121No ratings yet
- Eguide: Contamination Control in Pharmaceutical IndustryDocument17 pagesEguide: Contamination Control in Pharmaceutical Industrygsv988No ratings yet
- RABS and Isolators Barrier TechnologyDocument44 pagesRABS and Isolators Barrier TechnologySilke IgemannNo ratings yet
- QP-022 Sterilization Process ValidationDocument2 pagesQP-022 Sterilization Process Validationesraa asemNo ratings yet
- Sterility Assurance in PharmaceuticalsDocument24 pagesSterility Assurance in PharmaceuticalsDholakia100% (1)
- Multi Product Biopharmaceutical Manufacturing FacilitiesDocument18 pagesMulti Product Biopharmaceutical Manufacturing FacilitiesJason WangNo ratings yet
- Autoclave Validation PresentationDocument17 pagesAutoclave Validation PresentationprakhyaatNo ratings yet
- Microbiology and Sterility Assurance Book (2011)Document1 pageMicrobiology and Sterility Assurance Book (2011)Tim Sandle100% (1)
- Phuong - DryheatDocument5 pagesPhuong - DryheatqhpuongNo ratings yet
- Pharmaceutical Cleaning A Comprehensive Approach - 0Document15 pagesPharmaceutical Cleaning A Comprehensive Approach - 0Mina Maher MikhailNo ratings yet
- Most Frequently Asked Questions: Page 1 of 6Document66 pagesMost Frequently Asked Questions: Page 1 of 6shanmukha2007No ratings yet
- Instruction - SterilizationDocument36 pagesInstruction - SterilizationGiang100% (1)
- Smoke STUDIES ARTICLE 2 25 15 PDFDocument7 pagesSmoke STUDIES ARTICLE 2 25 15 PDFschumonNo ratings yet
- How To Successfully Implement A DisinfectantDocument2 pagesHow To Successfully Implement A DisinfectantTim Sandle100% (1)
- Testing Compressed Air Lines For Microbiological ContaminationDocument8 pagesTesting Compressed Air Lines For Microbiological Contaminationmuzammil21_adNo ratings yet
- Environmental Monitoring Performance QualificationDocument8 pagesEnvironmental Monitoring Performance Qualificationmehdi bahramiNo ratings yet
- Media Fills and Environment Atl Monitoring 26 July 2011 Presentation OneDocument18 pagesMedia Fills and Environment Atl Monitoring 26 July 2011 Presentation OneRiccardo TorelliNo ratings yet
- IVT Network - Sanitization of Pharmaceutical Facilities - 2014-08-29Document7 pagesIVT Network - Sanitization of Pharmaceutical Facilities - 2014-08-29Bhagath VikasNo ratings yet
- TRS 957 (2010) - Annex 3 - WHO GMP For Pharmaceutical Products Containing Hazardous SubstancesDocument17 pagesTRS 957 (2010) - Annex 3 - WHO GMP For Pharmaceutical Products Containing Hazardous SubstancesQuang Hiếu NgôNo ratings yet
- The Future of Systems Validation ACF1D6Document3 pagesThe Future of Systems Validation ACF1D6Mitchel JammalNo ratings yet
- USP 1228 DepyrogenationDocument5 pagesUSP 1228 Depyrogenationmustafa huseiny100% (1)
- Remington Chapter 40 SterilizationDocument26 pagesRemington Chapter 40 SterilizationAndhika Bintang Mahardhika50% (2)
- Ethylene Oxide Sterilization Process PDFDocument2 pagesEthylene Oxide Sterilization Process PDFJerry50% (2)
- BET CompleteDocument60 pagesBET CompleteKuldeepNo ratings yet
- DepyrogenationDocument7 pagesDepyrogenationOscar AyalaNo ratings yet
- Bio-Validation of Steam Sterilization - 758572676Document11 pagesBio-Validation of Steam Sterilization - 758572676venkats_001No ratings yet
- Pdajpst 2015 01079Document21 pagesPdajpst 2015 01079ErikaNo ratings yet
- Moist Heat Sterilization MythsDocument10 pagesMoist Heat Sterilization MythsmmyNo ratings yet
- 21122947Document6 pages21122947Victor CamargoNo ratings yet
- Validation of Process Gas SystemsDocument6 pagesValidation of Process Gas SystemsJuan Manuel Valdez Von FürthNo ratings yet
- Validation of Sterilization: GMP and Qa Class: BDocument50 pagesValidation of Sterilization: GMP and Qa Class: BHikmah Purnama AzaniNo ratings yet
- Autoclave Validation - What Is Really RequiredDocument4 pagesAutoclave Validation - What Is Really Requiredwadhwa_shailNo ratings yet
- Cleanroom Management in Pharmaceuticals and HealthcareDocument1 pageCleanroom Management in Pharmaceuticals and HealthcareTim SandleNo ratings yet
- Production of Plasma Proteins for Therapeutic UseFrom EverandProduction of Plasma Proteins for Therapeutic UseRating: 3 out of 5 stars3/5 (5)
- Sterilisation and Disinfection: Pharmaceutical MonographsFrom EverandSterilisation and Disinfection: Pharmaceutical MonographsRating: 5 out of 5 stars5/5 (3)
- Biocontamination Control for Pharmaceuticals and HealthcareFrom EverandBiocontamination Control for Pharmaceuticals and HealthcareRating: 5 out of 5 stars5/5 (1)
- Supplier Management in ETO Companies: An Analysis of Practices and ContingenciesDocument4 pagesSupplier Management in ETO Companies: An Analysis of Practices and ContingenciesSHAIK NISHARNo ratings yet
- Engineer-To-Order (ETO) Production Planning and Control: An Empirical Framework For Machinery-Building CompaniesDocument48 pagesEngineer-To-Order (ETO) Production Planning and Control: An Empirical Framework For Machinery-Building CompaniesSHAIK NISHARNo ratings yet
- Pharmaceutics 1st STERILIZATION Unit 4Document32 pagesPharmaceutics 1st STERILIZATION Unit 4SHAIK NISHARNo ratings yet
- Finite Element Analysis FormulasDocument19 pagesFinite Element Analysis FormulasSHAIK NISHARNo ratings yet
- Chapter - 1: Bicycle Operated Pedal Power Water PumpDocument37 pagesChapter - 1: Bicycle Operated Pedal Power Water PumpSHAIK NISHARNo ratings yet
- Diploma in Mechanical Engineering: Pedal Powered Water PumpDocument31 pagesDiploma in Mechanical Engineering: Pedal Powered Water PumpSHAIK NISHARNo ratings yet
- HMT FT Quiz-1Document2 pagesHMT FT Quiz-1Sweety VermaNo ratings yet
- JSS 1375-01-2004Document24 pagesJSS 1375-01-2004Loknath MathnikarNo ratings yet
- Chemistry Mcse PiDocument10 pagesChemistry Mcse PiMoses Samalani100% (1)
- 3 Cell RCPT ApparatusDocument13 pages3 Cell RCPT ApparatusBhupesh MulikNo ratings yet
- BS en 00438-4-2005 PDFDocument16 pagesBS en 00438-4-2005 PDFShan Sandaruwan AbeywardeneNo ratings yet
- GEA PowCoDocument35 pagesGEA PowCoSimon CaceresNo ratings yet
- 4529 Lase Shot PeeningDocument7 pages4529 Lase Shot PeeningcesarNo ratings yet
- CHM1 11 - 12 Q1 0605 FDDocument37 pagesCHM1 11 - 12 Q1 0605 FDkristan escananNo ratings yet
- Coconut Water Vinegar: New Alternative With Improved Processing TechniqueDocument10 pagesCoconut Water Vinegar: New Alternative With Improved Processing TechniqueJoel Nelson D'souza100% (1)
- 5.polymer ProfileDocument5 pages5.polymer ProfileLoki MrPerfectNo ratings yet
- Jiao2017 - Stomatal and Non-Stomatal Factors Regulated The Photosynthesis of Soybean Seedlings in The Present of Exogenous Bisphenol ADocument11 pagesJiao2017 - Stomatal and Non-Stomatal Factors Regulated The Photosynthesis of Soybean Seedlings in The Present of Exogenous Bisphenol AThông LêNo ratings yet
- Pendahuluan Ceramic MaterialsDocument45 pagesPendahuluan Ceramic MaterialsRaniNo ratings yet
- Diamant Technical Data Sheet Plasticmetal Model Ceram SetDocument4 pagesDiamant Technical Data Sheet Plasticmetal Model Ceram SetRogério FreitasNo ratings yet
- P - Block Reasoning 16, 17, 18 Very Simplified - (1) FDocument9 pagesP - Block Reasoning 16, 17, 18 Very Simplified - (1) FShazia FarheenNo ratings yet
- 08 - Chapter 1Document48 pages08 - Chapter 1danfm97No ratings yet
- Material Safety Data SheetDocument2 pagesMaterial Safety Data SheetarjunanpnNo ratings yet
- Er70S-2 Carbon Steel Welding Wire: Technical Specification SheetDocument2 pagesEr70S-2 Carbon Steel Welding Wire: Technical Specification Sheetrizviabbas2012No ratings yet
- Introduction To Numerical Methods in Chemical Engineering - P. AhujaDocument99 pagesIntroduction To Numerical Methods in Chemical Engineering - P. AhujaAnkit Kumar100% (2)
- Astm A666 - StainlesssteelDocument8 pagesAstm A666 - StainlesssteelPeter MohabNo ratings yet
- bài tập cuối kỳ 2Document17 pagesbài tập cuối kỳ 2KHÁNH VÕ ĐĂNGNo ratings yet
- Acothane Twin Pack: Product DescriptionDocument3 pagesAcothane Twin Pack: Product DescriptionpazhanivelmuruganNo ratings yet
- TDS Afff %3-En 1568Document2 pagesTDS Afff %3-En 1568JAKIR RONYNo ratings yet
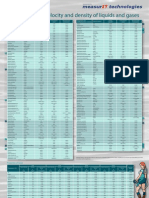
- MeasurIT Flexim Sound Velocity and Density 0910Document1 pageMeasurIT Flexim Sound Velocity and Density 0910cwiejkowskaNo ratings yet
- Paints Pigments and Industrial CoatingsDocument10 pagesPaints Pigments and Industrial CoatingsRaymond FuentesNo ratings yet
- Process Description1Document74 pagesProcess Description1mohsen ranjbarNo ratings yet
- Inorganic Chemistry 1 - Lesson 11 (Crystal Lattice and Lattice Energy)Document42 pagesInorganic Chemistry 1 - Lesson 11 (Crystal Lattice and Lattice Energy)bellaseba3_916194545No ratings yet
- Organic Chemistry Lab: Student ManualDocument62 pagesOrganic Chemistry Lab: Student ManualNguyễn AnNo ratings yet
- Title: Laboratory Activity: Viscosity of A LiquidDocument4 pagesTitle: Laboratory Activity: Viscosity of A LiquidMark John Paul CablingNo ratings yet




























































































You might also like
- PHSS Clarity On GMP Guidance No.3 Qualification of No Touch Transfer For RTU ContainersDocument8 pagesPHSS Clarity On GMP Guidance No.3 Qualification of No Touch Transfer For RTU ContainersAkuWilliamsNo ratings yet
- PHSS Control Strategy White PaperDocument13 pagesPHSS Control Strategy White PaperAkuWilliams100% (1)
- CCS Guide Attachment3 v2Document34 pagesCCS Guide Attachment3 v2elisabetta ghilardi100% (1)
- PDA Journal SeptemberDocument19 pagesPDA Journal SeptemberZia100% (2)
- Smoke Study Article 1Document15 pagesSmoke Study Article 1JAGADISH PHARMACEUTICALSNo ratings yet
- Tim Sandle White Paper EU - GMP - Annex - 1 - The - New - Draft - and - Implications 2020Document15 pagesTim Sandle White Paper EU - GMP - Annex - 1 - The - New - Draft - and - Implications 2020Supriya KapasNo ratings yet
- A Review of Cleanroom Microflora Types, Trends, and Patterns.Document14 pagesA Review of Cleanroom Microflora Types, Trends, and Patterns.Sean NamNo ratings yet
- 41 Sterilization Validation Key Steps To Dose Auditing 1Document2 pages41 Sterilization Validation Key Steps To Dose Auditing 1Vivian CerdasNo ratings yet
- S. No. SOP Title Room No. Responsibility StatusDocument1 pageS. No. SOP Title Room No. Responsibility Statusjpmaurya77No ratings yet
- Astm A668 Tensile ReqDocument1 pageAstm A668 Tensile ReqDilip Gajanan Namjoshi100% (1)
- Kleiberit PUR 501 - FISPQDocument8 pagesKleiberit PUR 501 - FISPQYuri SouzaNo ratings yet
- Use of Chemical & Biological Indicators - 2014 2Document56 pagesUse of Chemical & Biological Indicators - 2014 2jerimiah_manzonNo ratings yet
- PHSS - Clarity - in - GMP - Guidance - Barrier - Isolator - Technology - Leak Integrity Classes - v1Document12 pagesPHSS - Clarity - in - GMP - Guidance - Barrier - Isolator - Technology - Leak Integrity Classes - v1AkuWilliamsNo ratings yet
- ETO Sterilization ValidationDocument44 pagesETO Sterilization ValidationCRYSTAL2100100% (1)
- What Is Disinfectant ValidationDocument4 pagesWhat Is Disinfectant Validationrouss1906No ratings yet
- Multicenter Study On Incubation Conditions For Environmental Monitoring and Aseptic Process SimulationDocument9 pagesMulticenter Study On Incubation Conditions For Environmental Monitoring and Aseptic Process SimulationBLUEPRINT Integrated Engineering ServicesNo ratings yet
- General Chapters - 1222 - Terminally Sterilized Pharmaceutical Products-Parametric ReleaseDocument5 pagesGeneral Chapters - 1222 - Terminally Sterilized Pharmaceutical Products-Parametric ReleaseSuman Katteboina0% (1)
- RedBook BIT MayJune2012Document5 pagesRedBook BIT MayJune2012Liman SetiawanNo ratings yet
- Sanitization of Pharmaceutical FacilitiesDocument14 pagesSanitization of Pharmaceutical FacilitiesTim Sandle100% (1)
- Autoclave Validation: Presented by Paul Yeatman Bsc. MicrobiologistDocument17 pagesAutoclave Validation: Presented by Paul Yeatman Bsc. Microbiologistzfo302No ratings yet
- Cleanroom MicrobiologyDocument14 pagesCleanroom MicrobiologyKraken UrNo ratings yet
- 1231 - Water For Pharmaceutical PurposesDocument29 pages1231 - Water For Pharmaceutical PurposesLinh Nguyen100% (2)
- EO Annual Requalification ReviewDocument30 pagesEO Annual Requalification ReviewVenkatesh VenkateshNo ratings yet
- Guide For Determining The Confidence Interval Using ExcelDocument2 pagesGuide For Determining The Confidence Interval Using ExcelTim Sandle100% (3)
- IVT Network - Biodecontamination of Cleanrooms and Laboratories Using Gassing Systems - 2017-09-20Document13 pagesIVT Network - Biodecontamination of Cleanrooms and Laboratories Using Gassing Systems - 2017-09-20Le KhoaNo ratings yet
- Sterilization Validation QsiteDocument52 pagesSterilization Validation Qsiteskype2121No ratings yet
- Eguide: Contamination Control in Pharmaceutical IndustryDocument17 pagesEguide: Contamination Control in Pharmaceutical Industrygsv988No ratings yet
- RABS and Isolators Barrier TechnologyDocument44 pagesRABS and Isolators Barrier TechnologySilke IgemannNo ratings yet
- QP-022 Sterilization Process ValidationDocument2 pagesQP-022 Sterilization Process Validationesraa asemNo ratings yet
- Sterility Assurance in PharmaceuticalsDocument24 pagesSterility Assurance in PharmaceuticalsDholakia100% (1)
- Multi Product Biopharmaceutical Manufacturing FacilitiesDocument18 pagesMulti Product Biopharmaceutical Manufacturing FacilitiesJason WangNo ratings yet
- Autoclave Validation PresentationDocument17 pagesAutoclave Validation PresentationprakhyaatNo ratings yet
- Microbiology and Sterility Assurance Book (2011)Document1 pageMicrobiology and Sterility Assurance Book (2011)Tim Sandle100% (1)
- Phuong - DryheatDocument5 pagesPhuong - DryheatqhpuongNo ratings yet
- Pharmaceutical Cleaning A Comprehensive Approach - 0Document15 pagesPharmaceutical Cleaning A Comprehensive Approach - 0Mina Maher MikhailNo ratings yet
- Most Frequently Asked Questions: Page 1 of 6Document66 pagesMost Frequently Asked Questions: Page 1 of 6shanmukha2007No ratings yet
- Instruction - SterilizationDocument36 pagesInstruction - SterilizationGiang100% (1)
- Smoke STUDIES ARTICLE 2 25 15 PDFDocument7 pagesSmoke STUDIES ARTICLE 2 25 15 PDFschumonNo ratings yet
- How To Successfully Implement A DisinfectantDocument2 pagesHow To Successfully Implement A DisinfectantTim Sandle100% (1)
- Testing Compressed Air Lines For Microbiological ContaminationDocument8 pagesTesting Compressed Air Lines For Microbiological Contaminationmuzammil21_adNo ratings yet
- Environmental Monitoring Performance QualificationDocument8 pagesEnvironmental Monitoring Performance Qualificationmehdi bahramiNo ratings yet
- Media Fills and Environment Atl Monitoring 26 July 2011 Presentation OneDocument18 pagesMedia Fills and Environment Atl Monitoring 26 July 2011 Presentation OneRiccardo TorelliNo ratings yet
- IVT Network - Sanitization of Pharmaceutical Facilities - 2014-08-29Document7 pagesIVT Network - Sanitization of Pharmaceutical Facilities - 2014-08-29Bhagath VikasNo ratings yet
- TRS 957 (2010) - Annex 3 - WHO GMP For Pharmaceutical Products Containing Hazardous SubstancesDocument17 pagesTRS 957 (2010) - Annex 3 - WHO GMP For Pharmaceutical Products Containing Hazardous SubstancesQuang Hiếu NgôNo ratings yet
- The Future of Systems Validation ACF1D6Document3 pagesThe Future of Systems Validation ACF1D6Mitchel JammalNo ratings yet
- USP 1228 DepyrogenationDocument5 pagesUSP 1228 Depyrogenationmustafa huseiny100% (1)
- Remington Chapter 40 SterilizationDocument26 pagesRemington Chapter 40 SterilizationAndhika Bintang Mahardhika50% (2)
- Ethylene Oxide Sterilization Process PDFDocument2 pagesEthylene Oxide Sterilization Process PDFJerry50% (2)
- BET CompleteDocument60 pagesBET CompleteKuldeepNo ratings yet
- DepyrogenationDocument7 pagesDepyrogenationOscar AyalaNo ratings yet
- Bio-Validation of Steam Sterilization - 758572676Document11 pagesBio-Validation of Steam Sterilization - 758572676venkats_001No ratings yet
- Pdajpst 2015 01079Document21 pagesPdajpst 2015 01079ErikaNo ratings yet
- Moist Heat Sterilization MythsDocument10 pagesMoist Heat Sterilization MythsmmyNo ratings yet
- 21122947Document6 pages21122947Victor CamargoNo ratings yet
- Validation of Process Gas SystemsDocument6 pagesValidation of Process Gas SystemsJuan Manuel Valdez Von FürthNo ratings yet
- Validation of Sterilization: GMP and Qa Class: BDocument50 pagesValidation of Sterilization: GMP and Qa Class: BHikmah Purnama AzaniNo ratings yet
- Autoclave Validation - What Is Really RequiredDocument4 pagesAutoclave Validation - What Is Really Requiredwadhwa_shailNo ratings yet
- Cleanroom Management in Pharmaceuticals and HealthcareDocument1 pageCleanroom Management in Pharmaceuticals and HealthcareTim SandleNo ratings yet
- Production of Plasma Proteins for Therapeutic UseFrom EverandProduction of Plasma Proteins for Therapeutic UseRating: 3 out of 5 stars3/5 (5)
- Sterilisation and Disinfection: Pharmaceutical MonographsFrom EverandSterilisation and Disinfection: Pharmaceutical MonographsRating: 5 out of 5 stars5/5 (3)
- Biocontamination Control for Pharmaceuticals and HealthcareFrom EverandBiocontamination Control for Pharmaceuticals and HealthcareRating: 5 out of 5 stars5/5 (1)
- Supplier Management in ETO Companies: An Analysis of Practices and ContingenciesDocument4 pagesSupplier Management in ETO Companies: An Analysis of Practices and ContingenciesSHAIK NISHARNo ratings yet
- Engineer-To-Order (ETO) Production Planning and Control: An Empirical Framework For Machinery-Building CompaniesDocument48 pagesEngineer-To-Order (ETO) Production Planning and Control: An Empirical Framework For Machinery-Building CompaniesSHAIK NISHARNo ratings yet
- Pharmaceutics 1st STERILIZATION Unit 4Document32 pagesPharmaceutics 1st STERILIZATION Unit 4SHAIK NISHARNo ratings yet
- Finite Element Analysis FormulasDocument19 pagesFinite Element Analysis FormulasSHAIK NISHARNo ratings yet
- Chapter - 1: Bicycle Operated Pedal Power Water PumpDocument37 pagesChapter - 1: Bicycle Operated Pedal Power Water PumpSHAIK NISHARNo ratings yet
- Diploma in Mechanical Engineering: Pedal Powered Water PumpDocument31 pagesDiploma in Mechanical Engineering: Pedal Powered Water PumpSHAIK NISHARNo ratings yet
- HMT FT Quiz-1Document2 pagesHMT FT Quiz-1Sweety VermaNo ratings yet
- JSS 1375-01-2004Document24 pagesJSS 1375-01-2004Loknath MathnikarNo ratings yet
- Chemistry Mcse PiDocument10 pagesChemistry Mcse PiMoses Samalani100% (1)
- 3 Cell RCPT ApparatusDocument13 pages3 Cell RCPT ApparatusBhupesh MulikNo ratings yet
- BS en 00438-4-2005 PDFDocument16 pagesBS en 00438-4-2005 PDFShan Sandaruwan AbeywardeneNo ratings yet
- GEA PowCoDocument35 pagesGEA PowCoSimon CaceresNo ratings yet
- 4529 Lase Shot PeeningDocument7 pages4529 Lase Shot PeeningcesarNo ratings yet
- CHM1 11 - 12 Q1 0605 FDDocument37 pagesCHM1 11 - 12 Q1 0605 FDkristan escananNo ratings yet
- Coconut Water Vinegar: New Alternative With Improved Processing TechniqueDocument10 pagesCoconut Water Vinegar: New Alternative With Improved Processing TechniqueJoel Nelson D'souza100% (1)
- 5.polymer ProfileDocument5 pages5.polymer ProfileLoki MrPerfectNo ratings yet
- Jiao2017 - Stomatal and Non-Stomatal Factors Regulated The Photosynthesis of Soybean Seedlings in The Present of Exogenous Bisphenol ADocument11 pagesJiao2017 - Stomatal and Non-Stomatal Factors Regulated The Photosynthesis of Soybean Seedlings in The Present of Exogenous Bisphenol AThông LêNo ratings yet
- Pendahuluan Ceramic MaterialsDocument45 pagesPendahuluan Ceramic MaterialsRaniNo ratings yet
- Diamant Technical Data Sheet Plasticmetal Model Ceram SetDocument4 pagesDiamant Technical Data Sheet Plasticmetal Model Ceram SetRogério FreitasNo ratings yet
- P - Block Reasoning 16, 17, 18 Very Simplified - (1) FDocument9 pagesP - Block Reasoning 16, 17, 18 Very Simplified - (1) FShazia FarheenNo ratings yet
- 08 - Chapter 1Document48 pages08 - Chapter 1danfm97No ratings yet
- Material Safety Data SheetDocument2 pagesMaterial Safety Data SheetarjunanpnNo ratings yet
- Er70S-2 Carbon Steel Welding Wire: Technical Specification SheetDocument2 pagesEr70S-2 Carbon Steel Welding Wire: Technical Specification Sheetrizviabbas2012No ratings yet
- Introduction To Numerical Methods in Chemical Engineering - P. AhujaDocument99 pagesIntroduction To Numerical Methods in Chemical Engineering - P. AhujaAnkit Kumar100% (2)
- Astm A666 - StainlesssteelDocument8 pagesAstm A666 - StainlesssteelPeter MohabNo ratings yet
- bài tập cuối kỳ 2Document17 pagesbài tập cuối kỳ 2KHÁNH VÕ ĐĂNGNo ratings yet
- Acothane Twin Pack: Product DescriptionDocument3 pagesAcothane Twin Pack: Product DescriptionpazhanivelmuruganNo ratings yet
- TDS Afff %3-En 1568Document2 pagesTDS Afff %3-En 1568JAKIR RONYNo ratings yet
- MeasurIT Flexim Sound Velocity and Density 0910Document1 pageMeasurIT Flexim Sound Velocity and Density 0910cwiejkowskaNo ratings yet
- Paints Pigments and Industrial CoatingsDocument10 pagesPaints Pigments and Industrial CoatingsRaymond FuentesNo ratings yet
- Process Description1Document74 pagesProcess Description1mohsen ranjbarNo ratings yet
- Inorganic Chemistry 1 - Lesson 11 (Crystal Lattice and Lattice Energy)Document42 pagesInorganic Chemistry 1 - Lesson 11 (Crystal Lattice and Lattice Energy)bellaseba3_916194545No ratings yet
- Organic Chemistry Lab: Student ManualDocument62 pagesOrganic Chemistry Lab: Student ManualNguyễn AnNo ratings yet
- Title: Laboratory Activity: Viscosity of A LiquidDocument4 pagesTitle: Laboratory Activity: Viscosity of A LiquidMark John Paul CablingNo ratings yet