You might also like
- The Metabolic States Workbook: Track and Record Changes in Bodyweight and CompositionFrom EverandThe Metabolic States Workbook: Track and Record Changes in Bodyweight and CompositionNo ratings yet
- 1 Guidelines For Austere Conditions Introduction To Burn DisasterDocument21 pages1 Guidelines For Austere Conditions Introduction To Burn DisasterAlmas Nada SalsabilaNo ratings yet
- Name: Date Recorded: Measurements NotesDocument2 pagesName: Date Recorded: Measurements NotesANDROMEDANo ratings yet
- Management of Patient With BurnDocument52 pagesManagement of Patient With Burnrahul yadav100% (1)
- MC 1 Activity #1Document2 pagesMC 1 Activity #1Julienne Mae MillomedaNo ratings yet
- BURNSDocument27 pagesBURNSm.knirandaNo ratings yet
- TBSA Burn ChartDocument1 pageTBSA Burn ChartMaria Alexis Ahadain OlvidoNo ratings yet
- Dressmaking - Q2 - w2 DWHLPDocument3 pagesDressmaking - Q2 - w2 DWHLPSonia CanaNo ratings yet
- "How To Measure" Guide For Apparel Vendors 2009Document13 pages"How To Measure" Guide For Apparel Vendors 2009mohan smrNo ratings yet
- Bettas4all Standard2019 CaracteristicasGeneralesDocument5 pagesBettas4all Standard2019 CaracteristicasGeneralesoscarrodolfolopezNo ratings yet
- Critical Care - Burns - Top Missed QuestionsDocument1 pageCritical Care - Burns - Top Missed QuestionsKimberly Clarisse VegaNo ratings yet
- Basic Kid Wear For Girls. (Table)Document17 pagesBasic Kid Wear For Girls. (Table)Malakai sangmaNo ratings yet
- Universal Choking Sign: Viewgraph 1Document14 pagesUniversal Choking Sign: Viewgraph 1Mark CheneyNo ratings yet
- Activity 3: Practicing Using Correct Anatomical TerminologyDocument4 pagesActivity 3: Practicing Using Correct Anatomical TerminologyJocris Agasa CabaguanNo ratings yet
- Level 1 Workbook-Remedial Progressions-MinDocument5 pagesLevel 1 Workbook-Remedial Progressions-MinQuốc Huy100% (2)
- Blanko WeeFIM-Brain-InjuryDocument3 pagesBlanko WeeFIM-Brain-InjuryYusrina RahmaNo ratings yet
- Radiologic Examination of The Chest: KingwoodDocument88 pagesRadiologic Examination of The Chest: KingwoodClaudia BradleyNo ratings yet
- Body Orientation, Direction, Planes, and SectionsDocument2 pagesBody Orientation, Direction, Planes, and SectionsJenyeuxdeniniNo ratings yet
- Surface Anatomy Matching and Key TermsDocument2 pagesSurface Anatomy Matching and Key TermsJenyeuxdeniniNo ratings yet
- 20+2 Planes Eco IsuogDocument23 pages20+2 Planes Eco IsuogmarinaNo ratings yet
- Dr. Mike Israetel Training Volume Landmarks Hypertrophy RoutineDocument9 pagesDr. Mike Israetel Training Volume Landmarks Hypertrophy RoutineEmilyNo ratings yet
- Radiology and CT Scan for Diagnosing IllnessDocument6 pagesRadiology and CT Scan for Diagnosing IllnessAgus DorryNo ratings yet
- Asuna Overcoat Pattern by Yumelifecosplay d9c5r00Document1 pageAsuna Overcoat Pattern by Yumelifecosplay d9c5r00Fer MoraisNo ratings yet
- Oxford Emergency BurnsDocument16 pagesOxford Emergency BurnszahraaNo ratings yet
- Weefim Score Sheet: AmputationsDocument3 pagesWeefim Score Sheet: AmputationsDiedeeNo ratings yet
- Emergency and Disaster NursingDocument5 pagesEmergency and Disaster NursingreooooNo ratings yet
- Weefim BurnDocument3 pagesWeefim BurnDiedeeNo ratings yet
- AnthropometryDocument30 pagesAnthropometrySaqib AliNo ratings yet
- Laboratory Activity 1Document2 pagesLaboratory Activity 1sweetpeaNo ratings yet
- A Basic Pattern For You, Jane Speece, 1977Document9 pagesA Basic Pattern For You, Jane Speece, 1977Dan Andrei StefanNo ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document11 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Dian Permata PutraNo ratings yet
- Skinfold Measurement - 7 SiteDocument9 pagesSkinfold Measurement - 7 SiteRaja Nurul JannatNo ratings yet
- Ultrasound Notes For Trainees: DR Phurb DorjiDocument16 pagesUltrasound Notes For Trainees: DR Phurb DorjiooiziungieNo ratings yet
- Weefim Score Sheet: Brain InjuryDocument3 pagesWeefim Score Sheet: Brain InjuryDiedeeNo ratings yet
- Mechanism of Normal Labor: Presented byDocument68 pagesMechanism of Normal Labor: Presented byBharat ThapaNo ratings yet
- AlterationsDocument32 pagesAlterationsMaria RodriguezNo ratings yet
- Blazer Fitting EbookDocument31 pagesBlazer Fitting EbookMagnolia100% (1)
- Distinguishing Normal & Abnormal US Appearances of LimbsDocument29 pagesDistinguishing Normal & Abnormal US Appearances of LimbsBharti Pant GahtoriNo ratings yet
- 1501Document569 pages1501Ina Revenco33% (3)
- Measurements for Drafting Ladies Blouse PatternDocument17 pagesMeasurements for Drafting Ladies Blouse PatternadelfaNo ratings yet
- Malposition OcciputDocument29 pagesMalposition Occiputحسام رياض عبد الحسين راضيNo ratings yet
- Important For ExamDocument11 pagesImportant For ExamJagveer ChauhanNo ratings yet
- Burns Initial ManagementDocument4 pagesBurns Initial ManagementErnest Pardo RubioNo ratings yet
- Surface AnatomyDocument4 pagesSurface AnatomyZirah Lee ValledorNo ratings yet
- Anatomy & Physiology chicken and feather matching activityDocument3 pagesAnatomy & Physiology chicken and feather matching activitykierstyn cabalanNo ratings yet
- Operators Manual: BicepsDocument4 pagesOperators Manual: BicepsThomas SebastianiNo ratings yet
- 3.2 Joints GlandsDocument10 pages3.2 Joints GlandsrkNo ratings yet
- Littmann Pulmonary Auscultation PosterDocument1 pageLittmann Pulmonary Auscultation PosterHatim Haider AliNo ratings yet
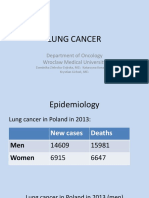
- Lung Cancer: Department of Oncology Wroclaw Medical UniversityDocument37 pagesLung Cancer: Department of Oncology Wroclaw Medical UniversityJuliaNo ratings yet
- Back Width 4. Upper Arm: 7. Armscye DepthDocument3 pagesBack Width 4. Upper Arm: 7. Armscye DepthSihem BedriNo ratings yet
- Pelvic AnatomyDocument106 pagesPelvic AnatomyRosu George100% (1)
- Rule of nines for burn percentageDocument2 pagesRule of nines for burn percentageVea Roanne GammadNo ratings yet
- Blazer Fitting EbookDocument31 pagesBlazer Fitting EbookDallexaorozco100% (2)
- Defender Instructions PDFDocument3 pagesDefender Instructions PDFKing DomNo ratings yet
- GyncDocument240 pagesGyncbolt boltNo ratings yet
- How To Make Your Own Bra and Lingerie (English)Document23 pagesHow To Make Your Own Bra and Lingerie (English)Siti Nur Intan L100% (4)
- Level 1 Workbook - Remedial Lifts-MinDocument4 pagesLevel 1 Workbook - Remedial Lifts-MinQuốc Huy100% (3)
- Dr. Mike Israetel Training Volume Landmarks Hypertrophy RoutineDocument24 pagesDr. Mike Israetel Training Volume Landmarks Hypertrophy RoutinepzphtcNo ratings yet
- Basic Bodice DraftingDocument18 pagesBasic Bodice DraftingLiyakath AliNo ratings yet
- IM Cardio - PERICARDIAL DISEASESDocument4 pagesIM Cardio - PERICARDIAL DISEASESElisha BernabeNo ratings yet
- Rule-In: Rule-Out: Reference: 1) SeizureDocument4 pagesRule-In: Rule-Out: Reference: 1) SeizureElisha BernabeNo ratings yet
- Through Typhoid Pharmacopeia. Diaphoresis Typhoid Produce: EnoughDocument6 pagesThrough Typhoid Pharmacopeia. Diaphoresis Typhoid Produce: EnoughElisha BernabeNo ratings yet
- Gallbladder Anatomy, Physiology, and DiseasesDocument33 pagesGallbladder Anatomy, Physiology, and DiseasesElisha BernabeNo ratings yet
- IM - Infective EndocarditisDocument11 pagesIM - Infective EndocarditisElisha Bernabe100% (1)
- IM - Heart Failure Part 1Document6 pagesIM - Heart Failure Part 1Elisha BernabeNo ratings yet
- IM - Infective EndocarditisDocument6 pagesIM - Infective EndocarditisElisha BernabeNo ratings yet
- IM - Cardiomyopathy and MyocarditisDocument9 pagesIM - Cardiomyopathy and MyocarditisElisha BernabeNo ratings yet
- IM - Heart Failure Part 2Document8 pagesIM - Heart Failure Part 2Elisha BernabeNo ratings yet
- IM - Pericardial DiseaseDocument6 pagesIM - Pericardial DiseaseElisha BernabeNo ratings yet
- IM - Cardiomyopathies and MyocarditisDocument8 pagesIM - Cardiomyopathies and MyocarditisElisha BernabeNo ratings yet
- Im 3B: Rheumatic Heart Disease: Far Eastern University - Nicanor Reyes Medical FoundationDocument4 pagesIm 3B: Rheumatic Heart Disease: Far Eastern University - Nicanor Reyes Medical FoundationChristian Jade A. BeatoNo ratings yet
- Media Media Media Media Media MediaDocument24 pagesMedia Media Media Media Media MediaElisha BernabeNo ratings yet
- Idsa Guidelines 2010Document32 pagesIdsa Guidelines 2010Angelo PadillaNo ratings yet
- Botany Botany Botany Botany Botany BotanyDocument1 pageBotany Botany Botany Botany Botany BotanyElisha BernabeNo ratings yet
- Cases Cases Cases CasesDocument4 pagesCases Cases Cases CasesElisha BernabeNo ratings yet
- Stanford Hospital & Clinics Antimicrobial Dosing Reference Guide 2013Document3 pagesStanford Hospital & Clinics Antimicrobial Dosing Reference Guide 2013SANCHOSKYNo ratings yet
- Rood Approach to Muscle Re-educationDocument33 pagesRood Approach to Muscle Re-educationRicha SoodNo ratings yet
- Antenatal CareDocument12 pagesAntenatal CarefiramnNo ratings yet
- @MBS MedicalBooksStore 2020 HeadDocument238 pages@MBS MedicalBooksStore 2020 HeadtamiNo ratings yet
- About The Measure Domain MeasureDocument3 pagesAbout The Measure Domain MeasureMaríaA.SerranoNo ratings yet
- Stop The Bleed Booklet FinalDocument16 pagesStop The Bleed Booklet FinalUrsula MalauNo ratings yet
- Food Poisoning and IntoxicationsDocument26 pagesFood Poisoning and IntoxicationslakshmijayasriNo ratings yet
- Placenta Accreta, Increta and PercretaDocument18 pagesPlacenta Accreta, Increta and Percretarutsanchez01No ratings yet
- Socket Shield Technique Vs Conventional Immediate Implant Placement With Immediate Temporization. Randomized Clinical TrialDocument10 pagesSocket Shield Technique Vs Conventional Immediate Implant Placement With Immediate Temporization. Randomized Clinical TrialeveraldocruzNo ratings yet
- Synovial ChondromatosisDocument4 pagesSynovial ChondromatosisNadia Bordaş100% (1)
- PATH Fit module on safety protocols and exercise health appraisalDocument1 pagePATH Fit module on safety protocols and exercise health appraisaljinNo ratings yet
- Europian Surgical Abstract 2 PDFDocument114 pagesEuropian Surgical Abstract 2 PDFDrAmmar MagdyNo ratings yet
- Braunwald - UA and NSTEMIDocument49 pagesBraunwald - UA and NSTEMIusfcards100% (2)
- Physical Health and Mental HealthDocument2 pagesPhysical Health and Mental HealthLuise MauieNo ratings yet
- Paraduodenal HerniaDocument4 pagesParaduodenal HerniadrhelNo ratings yet
- Question Preparation Exam-1-1Document281 pagesQuestion Preparation Exam-1-1SONGA AmriNo ratings yet
- Clinical Pathway Neonatal PneumoniaDocument4 pagesClinical Pathway Neonatal PneumoniaSHAINA ALIH. JUMAANINo ratings yet
- Introduction to Public Health NursingDocument37 pagesIntroduction to Public Health NursingKailash NagarNo ratings yet
- Fetal DistressDocument49 pagesFetal DistressLenny SucalditoNo ratings yet
- CBTDocument20 pagesCBTasharoopsing3No ratings yet
- Music TherapyDocument2 pagesMusic TherapytinaNo ratings yet
- ArikDocument14 pagesArikArditya Romy Stay CoolNo ratings yet
- EMR Implementation Readiness Assessment and Patient Satisfaction ReportDocument20 pagesEMR Implementation Readiness Assessment and Patient Satisfaction ReportAbidi HichemNo ratings yet
- Finasteride in Men With BPHDocument3 pagesFinasteride in Men With BPHmonia agni wiyatamiNo ratings yet
- General Stress Level of SHS ABM Students in Their Specialized SubjectDocument4 pagesGeneral Stress Level of SHS ABM Students in Their Specialized SubjectThons Nacu LisingNo ratings yet
- Cucms Rheumatology Questions PDFDocument3 pagesCucms Rheumatology Questions PDFMaisara JhsNo ratings yet
- Case Pres TamparanDocument22 pagesCase Pres TamparanAlano S. LimgasNo ratings yet
- Epilepsia EpicongressDocument245 pagesEpilepsia EpicongressВасилий КоптеловNo ratings yet
- Hospital Pharmacy Article Reviews Pregabalin for Neuropathic PainDocument16 pagesHospital Pharmacy Article Reviews Pregabalin for Neuropathic PainadityaNo ratings yet
- National Mental Health Programme Community Health NursingDocument17 pagesNational Mental Health Programme Community Health NursingLIDIYA MOL P V0% (1)