You might also like
- Smart-Ups On-Line Srt3000xla ApcDocument2 pagesSmart-Ups On-Line Srt3000xla ApcKatty CachagoNo ratings yet
- Guia CovidDocument4 pagesGuia CovidAndrés E. Espinoza NolascoNo ratings yet
- Dental Settings: Key ConceptsDocument7 pagesDental Settings: Key ConceptsVigneshvar SreekanthNo ratings yet
- Who 2019 Ncov Ipc Ppe Use 2020.3 EngDocument28 pagesWho 2019 Ncov Ipc Ppe Use 2020.3 EngKumanan1304No ratings yet
- 2020 Article 1361-2Document3 pages2020 Article 1361-2Maria Alejandra AconchaNo ratings yet
- Rational Use of Personal Protective Equipment (PPE) For Coronavirus Disease (COVID-19)Document9 pagesRational Use of Personal Protective Equipment (PPE) For Coronavirus Disease (COVID-19)Karthick AnbuNo ratings yet
- Recommendations For A Safety Dental Care Management During Sars-Cov-2 PandemicDocument4 pagesRecommendations For A Safety Dental Care Management During Sars-Cov-2 PandemicIoana CucuNo ratings yet
- Dental Care During The Coronavirus DiseaseDocument13 pagesDental Care During The Coronavirus DiseaseclinicNo ratings yet
- Guideline For Conservation of Respiratory Protection ResourcesDocument14 pagesGuideline For Conservation of Respiratory Protection ResourcesAMEU URGENCIASNo ratings yet
- COVID-19 Int Guidance Summary PDFDocument2 pagesCOVID-19 Int Guidance Summary PDFJavier NicolaldeNo ratings yet
- COVID-19 Int Guidance Summary PDFDocument2 pagesCOVID-19 Int Guidance Summary PDFShazeena QaiserNo ratings yet
- Kwak 2020Document4 pagesKwak 2020alyssaNo ratings yet
- BulletinDocument16 pagesBulletindean qpNo ratings yet
- Emergency Management in A Dental Clinic During TheDocument8 pagesEmergency Management in A Dental Clinic During TheAriska AndriyaniNo ratings yet
- ADA Managing COVID 19 Guide 25 March 2020Document6 pagesADA Managing COVID 19 Guide 25 March 2020Pepo BelovedNo ratings yet
- Approaches To The Management of Patients in Oral and Maxillofacial Surgery During COVID-19 PandemicDocument21 pagesApproaches To The Management of Patients in Oral and Maxillofacial Surgery During COVID-19 PandemicYahul MazfarNo ratings yet
- Apexa NO 8Document5 pagesApexa NO 8Apexa YadavNo ratings yet
- Sciencedirect: GuidelinesDocument4 pagesSciencedirect: Guidelinesanugraha GanendraNo ratings yet
- 2 Epitaxis Covid19Document3 pages2 Epitaxis Covid19andinNo ratings yet
- Covid19 Infection Prevention and ControlDocument70 pagesCovid19 Infection Prevention and ControlAdeuga ADEKUOYENo ratings yet
- Guidance On The Use of Personal Protective Equipment Ppe in Hospitals During The Covid 19 OutbreakDocument9 pagesGuidance On The Use of Personal Protective Equipment Ppe in Hospitals During The Covid 19 OutbreakGerlan Madrid MingoNo ratings yet
- Chen-2020-Preventive and Control Measures ForDocument6 pagesChen-2020-Preventive and Control Measures ForJaime GonzalezNo ratings yet
- WHO 2019 nCoV IPC 2021.1 EngDocument23 pagesWHO 2019 nCoV IPC 2021.1 Eng2110213 MUHAMMAD FARREL DANENDRANo ratings yet
- COVID 19 Guideline (Draft) of Bangladesh Dental Society: MethodDocument20 pagesCOVID 19 Guideline (Draft) of Bangladesh Dental Society: MethodMax FerNo ratings yet
- Update Who Recommendation On Covid-19 For Hospital: Setiawan Jati Laksono 10 April 2020Document34 pagesUpdate Who Recommendation On Covid-19 For Hospital: Setiawan Jati Laksono 10 April 2020Nadya FaradibaNo ratings yet
- DownloadDocument4 pagesDownloadSkAliHassanNo ratings yet
- Anaesthesia and Caring For Patients During The COVID-19 OutbreakDocument8 pagesAnaesthesia and Caring For Patients During The COVID-19 OutbreakMuhammad RenaldiNo ratings yet
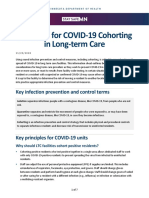
- Principles For COVID-19 Cohorting in Long-Term Care: Key Infection Prevention and Control TermsDocument7 pagesPrinciples For COVID-19 Cohorting in Long-Term Care: Key Infection Prevention and Control TermssimplyrosalynNo ratings yet
- Intensive Care Unit Setup For COVID-19Document10 pagesIntensive Care Unit Setup For COVID-19BAGUIO CATSNo ratings yet
- Review Article: COVID-19 Pandemic and Dental PracticeDocument5 pagesReview Article: COVID-19 Pandemic and Dental PracticeArevamadeline AegesfiNo ratings yet
- 10 1111@anae 15054 PDFDocument33 pages10 1111@anae 15054 PDFJuliana Rodriguez MariñoNo ratings yet
- Mask Use in The Context of COVID-19: Interim Guidance 1 December 2020Document22 pagesMask Use in The Context of COVID-19: Interim Guidance 1 December 2020ShahabNo ratings yet
- Mask Use in The Context of COVID-19: Interim Guidance 1 December 2020Document25 pagesMask Use in The Context of COVID-19: Interim Guidance 1 December 2020Ziyad BaraNo ratings yet
- WHO 2019 Ncov IPC - Masks 2020.5 EngDocument22 pagesWHO 2019 Ncov IPC - Masks 2020.5 EngsilviaNo ratings yet
- COVID-19: A Quick Look at Aspects of Critical CareDocument5 pagesCOVID-19: A Quick Look at Aspects of Critical CareJbarrianNo ratings yet
- Redefining Dental Practice During and Post-COVID-19 Era: A ReviewDocument9 pagesRedefining Dental Practice During and Post-COVID-19 Era: A Reviewapridey parinding08No ratings yet
- Intensive Care Unit Setup For COVID-19Document7 pagesIntensive Care Unit Setup For COVID-19BAGUIO CATSNo ratings yet
- LSUSDExposure Control Plan 2020Document53 pagesLSUSDExposure Control Plan 2020ILLYN TAPAYANo ratings yet
- Guidelines For Dental ServicesDocument6 pagesGuidelines For Dental Servicesdruzair007No ratings yet
- 2019 Novel Coronavirus (COVID-19) : Availability of Personal Protective EquipmentDocument4 pages2019 Novel Coronavirus (COVID-19) : Availability of Personal Protective EquipmentPetroNo ratings yet
- COVID 19 and ENT SurgeryDocument6 pagesCOVID 19 and ENT SurgeryYukiko CalimutanNo ratings yet
- Operational Considerations For COVID-19 Management in The Accommodation SectorDocument8 pagesOperational Considerations For COVID-19 Management in The Accommodation Sectorjorge Gregorio segura100% (1)
- WHO Masks GuidelinesDocument5 pagesWHO Masks GuidelinesLarryDCurtisNo ratings yet
- Running Title: Biosafety at The Dental Office After COVID-19Document16 pagesRunning Title: Biosafety at The Dental Office After COVID-19Karen IzquierdoNo ratings yet
- Covid19 Preventive Measures in The WorkplaceDocument8 pagesCovid19 Preventive Measures in The WorkplaceAnthony Sanglay, Jr.No ratings yet
- Covid Control and PreventionDocument8 pagesCovid Control and PreventionAlexadnerNo ratings yet
- Standard Operating Procedure For Handling of Corona Virus Disease (Covid-19) PatientsDocument6 pagesStandard Operating Procedure For Handling of Corona Virus Disease (Covid-19) PatientsHiJackNo ratings yet
- WHO 2019 Ncov IPC - Masks 2020.3 EngDocument5 pagesWHO 2019 Ncov IPC - Masks 2020.3 EngStephanie SommerfeldNo ratings yet
- ADA Interim Guidance For Minimizing Risk of COVID-19 TransmissionDocument8 pagesADA Interim Guidance For Minimizing Risk of COVID-19 TransmissionprasaddenNo ratings yet
- ADA COVID Int Guidance Treat Pts PDFDocument8 pagesADA COVID Int Guidance Treat Pts PDFJavier NicolaldeNo ratings yet
- ADA COVID Int Guidance Treat Pts 2 PDFDocument8 pagesADA COVID Int Guidance Treat Pts 2 PDFAnil SukumaranNo ratings yet
- ADA Interim Guidance For Minimizing Risk of COVID-19 TransmissionDocument8 pagesADA Interim Guidance For Minimizing Risk of COVID-19 TransmissionMaria Paula Vanegas ForeroNo ratings yet
- ADA Interim Guidance For Minimizing Risk of COVID-19 TransmissionDocument8 pagesADA Interim Guidance For Minimizing Risk of COVID-19 TransmissionOTNo ratings yet
- ADA COVID Int Guidance Treat Pts PDFDocument8 pagesADA COVID Int Guidance Treat Pts PDFFavio LunaNo ratings yet
- Covid Cat Ppe Masks 9 Revised 002Document8 pagesCovid Cat Ppe Masks 9 Revised 002semabayNo ratings yet
- ASA Staff Safety For COVID-19: StatementDocument8 pagesASA Staff Safety For COVID-19: StatementAbidi HichemNo ratings yet
- Impact of Coronavirus (COVID-19) On Otolaryngologic Surgery: Brief CommentaryDocument8 pagesImpact of Coronavirus (COVID-19) On Otolaryngologic Surgery: Brief CommentaryHesbon MomanyiNo ratings yet
- Infection Control Expert Group: The Use of Face Masks and Respirators in The Context of Covid-19Document24 pagesInfection Control Expert Group: The Use of Face Masks and Respirators in The Context of Covid-19Karen MooreNo ratings yet
- Clinical Endodontic Management During The COVID-19 Pandemic: A Literature Review and Clinical RecommendationsDocument11 pagesClinical Endodontic Management During The COVID-19 Pandemic: A Literature Review and Clinical Recommendationsangel gudiyaNo ratings yet
- China's Novel Coronavirus Response: Guidelines for Governments, Communities, Entities and Individuals to Combat COVID-19From EverandChina's Novel Coronavirus Response: Guidelines for Governments, Communities, Entities and Individuals to Combat COVID-19No ratings yet
- Receiving ElementDocument32 pagesReceiving ElementFELICIANO JOSE REYESNo ratings yet
- Complemento Uchile (Semigrupos)Document18 pagesComplemento Uchile (Semigrupos)robertoNo ratings yet
- Case Study With BIM - AECOM (Roseisle Distillery) PDFDocument2 pagesCase Study With BIM - AECOM (Roseisle Distillery) PDFRégis Lima SantanaNo ratings yet
- API 510 Open Book Practice ExamDocument48 pagesAPI 510 Open Book Practice Examcorey jacobsNo ratings yet
- Basic Operation and ControlsDocument109 pagesBasic Operation and Controlsluy nguyen100% (1)
- TableDocument10 pagesTableRome GentaNo ratings yet
- UM-DP12-25R UM-DP20-25R: The World's First Ultrasonic Probes With Dual-Plane Reconstruction Scanning CapabilityDocument3 pagesUM-DP12-25R UM-DP20-25R: The World's First Ultrasonic Probes With Dual-Plane Reconstruction Scanning CapabilityRicardo PaterninaNo ratings yet
- Marketing Management Project: Analysis On Tupperware ProductsDocument5 pagesMarketing Management Project: Analysis On Tupperware ProductsSakthi SaravananNo ratings yet
- CSPDCL-PV FormulaeDocument16 pagesCSPDCL-PV FormulaeAshish bhattNo ratings yet
- 9.6. V - N Diagram: From: Aircraft Performance Analysis, M. SadraeyDocument3 pages9.6. V - N Diagram: From: Aircraft Performance Analysis, M. SadraeyAbhiyan PaudelNo ratings yet
- Mahoney TableDocument3 pagesMahoney TablearpraveenneupaneNo ratings yet
- Tree Family & Common NameDocument4 pagesTree Family & Common NameJanine TugononNo ratings yet
- Epilepsy in ChildrenDocument34 pagesEpilepsy in ChildrenAdam MochtarNo ratings yet
- Cr976a - Westlake TyreDocument1 pageCr976a - Westlake TyreLuis Eduardo PuertoNo ratings yet
- Paper 4 - Structured QuestionsDocument20 pagesPaper 4 - Structured Questionsvita iftitahiyahNo ratings yet
- Carpentry ExamDocument2 pagesCarpentry ExamMelody Sarancial Sarial100% (1)
- Kinetics of Rectilinear MotionDocument12 pagesKinetics of Rectilinear MotionAyon SenguptaNo ratings yet
- 1 Diagram 1 Shows 2 Shaded Triangles and One Non-Shaded TriangleDocument21 pages1 Diagram 1 Shows 2 Shaded Triangles and One Non-Shaded TriangleCheran KumarNo ratings yet
- Transitivity & VoiceDocument24 pagesTransitivity & VoiceMiftahul SalamNo ratings yet
- Health Anxiety Module 6Document13 pagesHealth Anxiety Module 6madixxxxNo ratings yet
- Liquid-Penetrant-Testing-Level-1-Non-Destructive-Testing-And-Evaluation (Set 1)Document22 pagesLiquid-Penetrant-Testing-Level-1-Non-Destructive-Testing-And-Evaluation (Set 1)mishrateertharajNo ratings yet
- RF Basics GuideDocument92 pagesRF Basics GuideSandeep Reddy Vellapalem100% (2)
- STRAIGHT LINES (Cet)Document11 pagesSTRAIGHT LINES (Cet)Pratheek KeshavNo ratings yet
- Indigenous - Machinery - document-DAIRY PLANT PDFDocument197 pagesIndigenous - Machinery - document-DAIRY PLANT PDFkunal shahNo ratings yet
- Generator Type Eco 3-1Sn/4: Electrical CharacteristicsDocument5 pagesGenerator Type Eco 3-1Sn/4: Electrical CharacteristicsFaridh AmroullohNo ratings yet
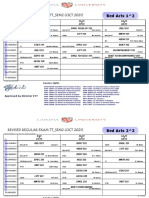
- Revised Regular Exam TT - Sem2 (Oct 2021) : Bed Arts 1 2Document78 pagesRevised Regular Exam TT - Sem2 (Oct 2021) : Bed Arts 1 2kelvinNo ratings yet
- EE3331C Feedback Control Systems L7: Control System Performance: Transient & Steady-StateDocument30 pagesEE3331C Feedback Control Systems L7: Control System Performance: Transient & Steady-Statepremsanjith subramaniNo ratings yet
- Introduction To Process ControlDocument29 pagesIntroduction To Process ControlSalih Ahmed ObeidNo ratings yet
- Spartacus To The Gladiators at Capua: A Monologue by E. KelloggDocument2 pagesSpartacus To The Gladiators at Capua: A Monologue by E. KelloggDanny SethNo ratings yet