You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Complete Guide To Home CompostingDocument79 pagesComplete Guide To Home CompostingJoaquin Chila FNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- SONY XBR-55X850C - XBR-55X855C - XBR-55X857C - XBR-65X850C - Ch. - GN1T PDFDocument217 pagesSONY XBR-55X850C - XBR-55X855C - XBR-55X857C - XBR-65X850C - Ch. - GN1T PDFboroda2410No ratings yet
- BS en 12464 1 Lighting Levels PDFDocument3 pagesBS en 12464 1 Lighting Levels PDFGUNABALAN100% (1)
- Third Point Investor PresentationDocument29 pagesThird Point Investor PresentationValueWalkNo ratings yet
- Action Flows A320Document13 pagesAction Flows A320SS Malik100% (2)
- Chapter 8: "Work Stress Kills"Document2 pagesChapter 8: "Work Stress Kills"dangNo ratings yet
- WBS - Friends and Family Party - BlankDocument2 pagesWBS - Friends and Family Party - BlankUltimat MaranhaoNo ratings yet
- Literature Review of Zinc OxideDocument6 pagesLiterature Review of Zinc Oxidebsdavcvkg100% (1)
- Considerations On The Use of Air - Lift Pumps in The Sewage Treatment PlantsDocument7 pagesConsiderations On The Use of Air - Lift Pumps in The Sewage Treatment PlantsvladmmuresanNo ratings yet
- ESPCP General Notes TemplateDocument13 pagesESPCP General Notes TemplateKhairil AjjaNo ratings yet
- Quality Assurance Plan For Ptfe Lined Pipes & FittingsDocument1 pageQuality Assurance Plan For Ptfe Lined Pipes & Fittingsروشان فاطمة روشانNo ratings yet
- Assignment-1 (2020011108)Document28 pagesAssignment-1 (2020011108)Atul KumarNo ratings yet
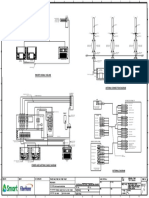
- Rbs/Bts Signal Cabling: DF PanelDocument1 pageRbs/Bts Signal Cabling: DF PanelMayuSalanggaNo ratings yet
- Proposal For Improvement of Infant Toddler Weighing ScaleDocument6 pagesProposal For Improvement of Infant Toddler Weighing ScaleYuna-chan KatsuraNo ratings yet
- Ged Life Science Question PaperDocument9 pagesGed Life Science Question Papermallikammu12No ratings yet
- 1.1 HSE Policy 2018 MergedDocument133 pages1.1 HSE Policy 2018 MergedMohamed RizwanNo ratings yet
- Samsung UN75J6300 UWK50 PDFDocument86 pagesSamsung UN75J6300 UWK50 PDFautreraNo ratings yet
- ChocolateDocument2 pagesChocolateJose Francisco Meneses SoteloNo ratings yet
- Clinical NutritionDocument108 pagesClinical Nutritionakoeljames8543No ratings yet
- One Form Should Be Completed by An Adult Member of Each Family. Print in Capital (UPPERCASE) Letters. Leave Blank Boxes For SpacesDocument1 pageOne Form Should Be Completed by An Adult Member of Each Family. Print in Capital (UPPERCASE) Letters. Leave Blank Boxes For Spacesfloryfloryy4281No ratings yet
- Autocan Vag ManualDocument42 pagesAutocan Vag ManualHumbertoNo ratings yet
- Manual de Operación ONANDocument37 pagesManual de Operación ONANFernando PadillaNo ratings yet
- The Role of Working Memory in SportDocument25 pagesThe Role of Working Memory in SportChrisNo ratings yet
- Orthopedics NCPDocument2 pagesOrthopedics NCPRene Gabriel FernandoNo ratings yet
- Increase Op-Amp Output Voltage Swing Boosting OutputDocument7 pagesIncrease Op-Amp Output Voltage Swing Boosting OutputmammolloNo ratings yet
- Sonia Thakker 184 Jignesh Bhatt 105 Rekha Wachkawde 188 Shailendra Singh 178 Pravin Nayak 147 Jibu James 128Document44 pagesSonia Thakker 184 Jignesh Bhatt 105 Rekha Wachkawde 188 Shailendra Singh 178 Pravin Nayak 147 Jibu James 128treakoNo ratings yet
- Colegio Santo Ángel de La Guarda: 180 Años de Presencia AngelinaDocument5 pagesColegio Santo Ángel de La Guarda: 180 Años de Presencia AngelinaJexDv16No ratings yet
- Assignment 2Document31 pagesAssignment 2Asim UstadNo ratings yet
- Marketing EnvironmentDocument23 pagesMarketing EnvironmentSudu PuthaNo ratings yet
- Slide Via 14 SeptDocument78 pagesSlide Via 14 SeptLAWANYA A/P LETCHUMANAN MoeNo ratings yet