You might also like
- CML, CLLDocument118 pagesCML, CLLMunesh SherawatNo ratings yet
- Diseases of White Blood Cells and Lymph NodesDocument105 pagesDiseases of White Blood Cells and Lymph NodesMario De la Fuente100% (1)
- Haematopathology 3:: Leucocytosis/LeucopeniaDocument113 pagesHaematopathology 3:: Leucocytosis/LeucopeniaarwaNo ratings yet
- Understanding Acute and Chronic LeukemiaDocument10 pagesUnderstanding Acute and Chronic LeukemiaKrisha BalorioNo ratings yet
- Fast Facts: Measurable Residual Disease: A clearer picture for treatment decisionsFrom EverandFast Facts: Measurable Residual Disease: A clearer picture for treatment decisionsNo ratings yet
- Leukocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandLeukocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- BoardReviewPart2B MalignantHemePathDocument207 pagesBoardReviewPart2B MalignantHemePathMaria Cristina Alarcon NietoNo ratings yet
- Chronic Myeloid Leukemia DiagnosisDocument4 pagesChronic Myeloid Leukemia DiagnosisKarl Jimenez SeparaNo ratings yet
- Understanding Non-Hodgkins Lymphoma: Classification, Risk Factors, PresentationDocument95 pagesUnderstanding Non-Hodgkins Lymphoma: Classification, Risk Factors, PresentationwihelminaNo ratings yet
- A Pattern Based Approach To Nodal Lymphoma: The Critical Role of HistologyDocument55 pagesA Pattern Based Approach To Nodal Lymphoma: The Critical Role of Histologylazy19No ratings yet
- Myelodysplastic Syndromes Hematology 1: 1. MDS With Multilineage Dysplasia (MDS-MLD)Document9 pagesMyelodysplastic Syndromes Hematology 1: 1. MDS With Multilineage Dysplasia (MDS-MLD)Joezer Gumangan VeranoNo ratings yet
- LABORATORY MEASUREMENTS OF PLATELET ACTIVITIESDocument73 pagesLABORATORY MEASUREMENTS OF PLATELET ACTIVITIESMary Lyka ReyesNo ratings yet
- The Importance of Considering Thalassaemia in Low MCV or MCH Blood CountsDocument40 pagesThe Importance of Considering Thalassaemia in Low MCV or MCH Blood CountsHenni Junita Siregar SorminNo ratings yet
- Red Cell and White Cell Counting, BloodDocument89 pagesRed Cell and White Cell Counting, BloodJovel GangcuangcoNo ratings yet
- Guide To Clinical Management of Idiopathic Pulmonary FibrosisDocument135 pagesGuide To Clinical Management of Idiopathic Pulmonary FibrosisConstantin PopescuNo ratings yet
- Taxotere Docetaxel 80 mg/4 ML Concentrate For Solution For InfusionDocument52 pagesTaxotere Docetaxel 80 mg/4 ML Concentrate For Solution For InfusionArbiati Rahman100% (1)
- Diagnosis and Management of Plasma Cell DisordersDocument23 pagesDiagnosis and Management of Plasma Cell Disordersbubbu92No ratings yet
- WBC BasicsDocument70 pagesWBC BasicsZoe ZillaNo ratings yet
- Department of Pathology, Dhanalakshmi Srinivasan Medical College and Hospital, Siruvachur, Perambalur, Tamil Nadu, IndiaDocument14 pagesDepartment of Pathology, Dhanalakshmi Srinivasan Medical College and Hospital, Siruvachur, Perambalur, Tamil Nadu, IndiaaishaNo ratings yet
- Physical Examination of Urine: Analysis of Urine and Other Body Fluids Module 4Document19 pagesPhysical Examination of Urine: Analysis of Urine and Other Body Fluids Module 4Francis ValdezNo ratings yet
- Managing Febrile Neutropenia in Pediatric Oncology PatientsDocument38 pagesManaging Febrile Neutropenia in Pediatric Oncology Patientsdr FAHADKHALIQSIALNo ratings yet
- Cancer ChemotherapyDocument86 pagesCancer ChemotherapyFrancheska MicuNo ratings yet
- CP - Hemophilia 2Document40 pagesCP - Hemophilia 2Reezka PutraNo ratings yet
- Leukocyte DisordersDocument55 pagesLeukocyte DisordersSherlyn Yee100% (1)
- HPLC PPT - KarishmaDocument76 pagesHPLC PPT - KarishmaDivya GauravNo ratings yet
- Hematopoietic SystemDocument39 pagesHematopoietic SystemapplesncoreNo ratings yet
- Bone Marrow Morphology: Normal and Abnormal FindingsDocument51 pagesBone Marrow Morphology: Normal and Abnormal FindingsMohammed FareedNo ratings yet
- Acute Lymphoblastic Leukemia QuestionsDocument22 pagesAcute Lymphoblastic Leukemia Questionsđoàn lươngNo ratings yet
- Megaloblastic Anemia Testing AlgorithmDocument1 pageMegaloblastic Anemia Testing AlgorithmkatNo ratings yet
- Red Blood Cell Disorders Anemia: Anemia Is A Laboratory DiagnosisDocument3 pagesRed Blood Cell Disorders Anemia: Anemia Is A Laboratory DiagnosisAnonymous 8hJAATBNo ratings yet
- Hematology OncologyDocument476 pagesHematology OncologySukumar SubramaniNo ratings yet
- Faquin Milian System and Molecular Advances in Diagnosis Salivary Gland TumorsDocument87 pagesFaquin Milian System and Molecular Advances in Diagnosis Salivary Gland TumorsJoanna Marie100% (1)
- (6-7) PATH - Colonic Polyps and CarcinomaDocument11 pages(6-7) PATH - Colonic Polyps and Carcinomaaaron mbindyoNo ratings yet
- Top 10 Anemias to Know for BoardsDocument24 pagesTop 10 Anemias to Know for BoardsSim M ChangNo ratings yet
- Multiple Myeloma: Presented By: DR - Ramesh Kumar Guide:-Dr. O.P. Meena SirDocument65 pagesMultiple Myeloma: Presented By: DR - Ramesh Kumar Guide:-Dr. O.P. Meena Sirvikash meenaNo ratings yet
- MUST To KNOW in Hematology1-1Document45 pagesMUST To KNOW in Hematology1-1Jez Mendoza ManuelNo ratings yet
- Lymphoproliferative disorders diagnosis and treatmentDocument29 pagesLymphoproliferative disorders diagnosis and treatmentShaza ElkourashyNo ratings yet
- Is My Patient "Drug-Seeking"?: Matthew Hathaway Courtney Samanipour Amanda SeedsDocument12 pagesIs My Patient "Drug-Seeking"?: Matthew Hathaway Courtney Samanipour Amanda Seedsapi-284053760No ratings yet
- Interpretation of Liver Enzyme Tests - A Rapid GuideDocument3 pagesInterpretation of Liver Enzyme Tests - A Rapid Guidesserggios100% (2)
- Anemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDocument15 pagesAnemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDanielle FosterNo ratings yet
- Introduction To TransplantationDocument3 pagesIntroduction To TransplantationGerardLumNo ratings yet
- Leukaemia and Lymphoma Whats The DifferenceDocument7 pagesLeukaemia and Lymphoma Whats The Differencepaul_calburean7899No ratings yet
- Lymphoma Diagnosis BCSH 042010Document59 pagesLymphoma Diagnosis BCSH 042010DR_Alaa_FakhriNo ratings yet
- Hema Part 3 Final PDFDocument188 pagesHema Part 3 Final PDFH.B.ANo ratings yet
- Molecular Diagnosis in HaematologyDocument23 pagesMolecular Diagnosis in HaematologyUmar'Farouq Oni100% (1)
- Carboplatin PaclitaxelDocument6 pagesCarboplatin PaclitaxelNida Auliya RahmahNo ratings yet
- Lymphoid NeoplasmsDocument52 pagesLymphoid NeoplasmsAmalia Riska GNo ratings yet
- MMDocument67 pagesMMRatnaNo ratings yet
- AML Pita DR MardiahDocument71 pagesAML Pita DR MardiahSarly Puspita AriesaNo ratings yet
- Tumor Markeri - Eng PDFDocument79 pagesTumor Markeri - Eng PDFdr_4uNo ratings yet
- CELL OVERVIEW PREVENTION Notes 2015Document7 pagesCELL OVERVIEW PREVENTION Notes 2015Alexander LukashenkoNo ratings yet
- Myeloproliferative Disorders (MPD) : Pathogenesis Clinical Laboratory FindingsDocument2 pagesMyeloproliferative Disorders (MPD) : Pathogenesis Clinical Laboratory FindingskakuNo ratings yet
- Diagnosis and Treatment of Multiple MyelomaDocument40 pagesDiagnosis and Treatment of Multiple MyelomaHula HulahulagNo ratings yet
- BCCA Febrile Neutropenia GuidelinesDocument2 pagesBCCA Febrile Neutropenia GuidelinesdenokayuMRNo ratings yet
- FRCPath+picture-based+questions (1)Document39 pagesFRCPath+picture-based+questions (1)Marvi UmairNo ratings yet
- WBC Lymph Node SpleenDocument12 pagesWBC Lymph Node Spleendr brijesh TiwariNo ratings yet
- AAK ANA Komplett Kunde PDFDocument64 pagesAAK ANA Komplett Kunde PDFm parasiteNo ratings yet
- Urinary Tract Infection: ClassificationDocument8 pagesUrinary Tract Infection: ClassificationMaram AbdullahNo ratings yet
- financial analysis project and rubricDocument3 pagesfinancial analysis project and rubricMaram AbdullahNo ratings yet
- Fundamentals of Management, 7e (Robbins/DeCenzo/Coulter)Document47 pagesFundamentals of Management, 7e (Robbins/DeCenzo/Coulter)Ebtehal TamerNo ratings yet
- Course outline_Fall 2024 (1)Document5 pagesCourse outline_Fall 2024 (1)Maram AbdullahNo ratings yet
- Pre Marital Counseling MMMDocument90 pagesPre Marital Counseling MMMMaram AbdullahNo ratings yet
- Peads HistoryDocument2 pagesPeads Historyapi-349464568No ratings yet
- Structured Oral Exam (SOE) - Mock Exam Checklist: Theme: Medication Safety in Outpatient SettingDocument2 pagesStructured Oral Exam (SOE) - Mock Exam Checklist: Theme: Medication Safety in Outpatient SettingMaram AbdullahNo ratings yet
- Approach To HematuriaDocument3 pagesApproach To HematuriaMaram AbdullahNo ratings yet
- NIHMS783367 Supplement SupplementalDocument15 pagesNIHMS783367 Supplement SupplementalMaram AbdullahNo ratings yet
- Pcos GP Tool 2dec2013Document6 pagesPcos GP Tool 2dec2013Maram AbdullahNo ratings yet
- Centor ScoreDocument8 pagesCentor ScoreLoo DonNo ratings yet
- Jurnal TelingaDocument7 pagesJurnal TelingaanaaNo ratings yet
- Nice For Hearing LossDocument17 pagesNice For Hearing LossMaram AbdullahNo ratings yet
- Audiometry Screening and Interpretation Aafp PDFDocument8 pagesAudiometry Screening and Interpretation Aafp PDFMaram AbdullahNo ratings yet
- Otits Externa BMJDocument44 pagesOtits Externa BMJMaram AbdullahNo ratings yet
- Understanding Your Child's AudiogramDocument1 pageUnderstanding Your Child's AudiogramMaram Abdullah100% (1)
- AAO-HNS Releases Guideline On Sudden Hearing LossDocument3 pagesAAO-HNS Releases Guideline On Sudden Hearing LossMaram AbdullahNo ratings yet
- 2 Anxiety Disorders MineDocument46 pages2 Anxiety Disorders MineMaram AbdullahNo ratings yet
- Common Vulval DermatosesDocument6 pagesCommon Vulval DermatosesMaram AbdullahNo ratings yet
- WHO SugarGuidelinesDocument59 pagesWHO SugarGuidelinesMaram AbdullahNo ratings yet
- Peds 2017-0967 FullDocument10 pagesPeds 2017-0967 FullNithin OmanakuttanNo ratings yet
- Antibiotics: Choices For Common InfectionsDocument30 pagesAntibiotics: Choices For Common InfectionsAlfeus GradyNo ratings yet
- JNC 8 Guideline Algorithm for Treating HypertensionDocument2 pagesJNC 8 Guideline Algorithm for Treating HypertensionTaradifaNurInsi0% (1)
- JNC 8 Guideline Algorithm for Treating HypertensionDocument2 pagesJNC 8 Guideline Algorithm for Treating HypertensionTaradifaNurInsi0% (1)
- 14 Renal Stone, Hydronephrosis, &polycystic KDocument33 pages14 Renal Stone, Hydronephrosis, &polycystic KMaram AbdullahNo ratings yet
- JNC 8 Guideline Algorithm for Treating HypertensionDocument2 pagesJNC 8 Guideline Algorithm for Treating HypertensionTaradifaNurInsi0% (1)
- PB 4Document3 pagesPB 4Maram AbdullahNo ratings yet
- PBL 2Document3 pagesPBL 2Maram AbdullahNo ratings yet
- Differential Diagnosis of Brittle HairDocument1 pageDifferential Diagnosis of Brittle HairMaram AbdullahNo ratings yet
- NIH CancerDocument198 pagesNIH CancerAnonymous KgUtPlkjNo ratings yet
- Oncology Drugs in the Pipeline ChartDocument17 pagesOncology Drugs in the Pipeline Chartjessiliang9No ratings yet
- Essentials of Internal MedicineDocument832 pagesEssentials of Internal MedicineEmanuelMC100% (75)
- Pedia 102 Quiz 2 SemifinalsDocument19 pagesPedia 102 Quiz 2 Semifinalsquidditch07100% (1)
- EvolDocument11 pagesEvolpharmaNo ratings yet
- Tin LeukemiaDocument15 pagesTin LeukemiaKristine YoungNo ratings yet
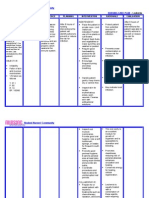
- Nursing Care Plan LeukemiaDocument2 pagesNursing Care Plan Leukemiaderic87% (30)
- 02 Family Medicine Answer Key PDFDocument5 pages02 Family Medicine Answer Key PDFJennifer Pisco LiracNo ratings yet
- E. DOCK 8 DeficiencyDocument22 pagesE. DOCK 8 DeficiencyAseel AliNo ratings yet
- IJIACS Paper CorrectedDocument7 pagesIJIACS Paper CorrectedArnabesh DasNo ratings yet
- Drugs in Medicine by Medad Team FinalDocument5 pagesDrugs in Medicine by Medad Team Finalعبد الرحمن100% (2)
- Me Earl The Dying GirlDocument125 pagesMe Earl The Dying GirlJosh CornejoNo ratings yet
- SP ACCURE InjectablesDocument8 pagesSP ACCURE Injectablessanjay_gawaliNo ratings yet
- Portola Middle School: Ochsa: Writing ConservatoryDocument20 pagesPortola Middle School: Ochsa: Writing ConservatoryTedNo ratings yet
- Limfoma (Kuliah 3a Ipd III)Document30 pagesLimfoma (Kuliah 3a Ipd III)Rianda Dwi PutraNo ratings yet
- 37 Report PDFDocument39 pages37 Report PDFadnanNo ratings yet
- Paulding County Progress June 1, 2011Document16 pagesPaulding County Progress June 1, 2011PauldingProgressNo ratings yet
- Pediatric Oncology Quiz: Key Facts about Childhood Cancers and Their TreatmentDocument22 pagesPediatric Oncology Quiz: Key Facts about Childhood Cancers and Their TreatmentFull MarksNo ratings yet
- Leukemia Infographic PDFDocument1 pageLeukemia Infographic PDFPriyanka KhuranaNo ratings yet
- Cytogenetics Final ExamDocument20 pagesCytogenetics Final ExamMICHAEL JOHN AGUILARNo ratings yet
- Childhood Acute Myeloid Leukaemia (AML) : A Guide For ParentsDocument32 pagesChildhood Acute Myeloid Leukaemia (AML) : A Guide For ParentsJennyNo ratings yet
- Protocol Outline Remission Induction (6-7 Weeks)Document3 pagesProtocol Outline Remission Induction (6-7 Weeks)Mohammed HaiderNo ratings yet
- Intron A: Escherichia ColiDocument44 pagesIntron A: Escherichia ColiAristoteles Esteban Cine VelazquezNo ratings yet
- Acute Myeloid LeukemiaDocument33 pagesAcute Myeloid LeukemiardLuis1No ratings yet
- Barrie Trower Wifi Report - Humanity at The BrinkDocument8 pagesBarrie Trower Wifi Report - Humanity at The Brinkcurtycurt01No ratings yet
- Hematology exam answers and correctionsDocument57 pagesHematology exam answers and correctionsOng Christopher100% (2)
- Under Funded Cancers: A Review of LiteratureDocument11 pagesUnder Funded Cancers: A Review of Literatureapi-301349510No ratings yet
- Adult Acute Lymphoblastic LeukemiaDocument22 pagesAdult Acute Lymphoblastic Leukemiamelki hadisasmitaNo ratings yet
- Molecular Pathology of Hematolymphoid Diseases - C. Dunphy (Springer, 2010) WW PDFDocument613 pagesMolecular Pathology of Hematolymphoid Diseases - C. Dunphy (Springer, 2010) WW PDFMoldovan Tiberiu100% (2)