You might also like
- Is Coracoclavicular Reconstruction Necessary in Hook Plate Fixation For Acute Unstable Acromioclavicular Dislocation?Document11 pagesIs Coracoclavicular Reconstruction Necessary in Hook Plate Fixation For Acute Unstable Acromioclavicular Dislocation?Yuni NatasyaNo ratings yet
- Revisão Anatomica e Biomecanica - 2023Document14 pagesRevisão Anatomica e Biomecanica - 2023Tayllane SantosNo ratings yet
- Acl Bone Graft With Mini ArthrotomyDocument9 pagesAcl Bone Graft With Mini Arthrotomypaper coe medanNo ratings yet
- Slight Femoral Under-Correction Versus Neutral Alignment in Total Knee Arthroplasty With Preoperative Varus Knees: A Comparative StudyDocument8 pagesSlight Femoral Under-Correction Versus Neutral Alignment in Total Knee Arthroplasty With Preoperative Varus Knees: A Comparative Studyfebyan yohanesNo ratings yet
- Allograft Acl 2012Document12 pagesAllograft Acl 2012Phooi Yee LauNo ratings yet
- Distal Humeral Fractures-Current Concepts PDFDocument11 pagesDistal Humeral Fractures-Current Concepts PDFRina AlvionitaNo ratings yet
- He 2019Document10 pagesHe 2019Rashif AkmalNo ratings yet
- Research Pankaj Tunnel ImportanceDocument7 pagesResearch Pankaj Tunnel Importancerakhee soniNo ratings yet
- Rehabilitation Program: Physical TherapyDocument3 pagesRehabilitation Program: Physical TherapyEffendi UChinNo ratings yet
- The Relationship Between Anterior Cruciate Ligament Injury and Osteoarthritis of The KneeDocument12 pagesThe Relationship Between Anterior Cruciate Ligament Injury and Osteoarthritis of The KneeMufidAljaruNo ratings yet
- Studyprotocol Open AccessDocument9 pagesStudyprotocol Open AccessKarthikeyan DNo ratings yet
- Cortical Mandibular Bone Blocks Grafts and Piezoelectric Surgery in Complex Anterior Maxillary Alveolar Defects A Case Report and Literature ReviewDocument6 pagesCortical Mandibular Bone Blocks Grafts and Piezoelectric Surgery in Complex Anterior Maxillary Alveolar Defects A Case Report and Literature ReviewAthenaeum Scientific PublishersNo ratings yet
- Comparison of The Modified Transtibial Technique, Anteromedial Portal Technique and Outside-In Technique in ACL ReconstructionDocument8 pagesComparison of The Modified Transtibial Technique, Anteromedial Portal Technique and Outside-In Technique in ACL ReconstructionJahid HasanNo ratings yet
- JCM 10 00912 v2Document12 pagesJCM 10 00912 v2Luthfi LazuardiNo ratings yet
- Orthopaedic Surgery - 2023 - Wang - Comparison of Robot Assisted Percutaneous Cannulated Screws Versus Open Reduction andDocument7 pagesOrthopaedic Surgery - 2023 - Wang - Comparison of Robot Assisted Percutaneous Cannulated Screws Versus Open Reduction andOnSolomonNo ratings yet
- 12 2019 Ring VS Tent 2019Document10 pages12 2019 Ring VS Tent 2019feli.riam24No ratings yet
- ACL BrotzmanDocument7 pagesACL Brotzmankhushboopakhrani98No ratings yet
- How To Achieve An Optimal Alignment in Medial Opening Wedge High Tibial Osteotomy?Document11 pagesHow To Achieve An Optimal Alignment in Medial Opening Wedge High Tibial Osteotomy?陳韋傑No ratings yet
- 1348 6456 4 PBDocument7 pages1348 6456 4 PB林良駿No ratings yet
- MatthewVaracalloMD TotalKneeReplacementTKRTechniques StatPearls NCBIBookshelfDocument14 pagesMatthewVaracalloMD TotalKneeReplacementTKRTechniques StatPearls NCBIBookshelfDiego Alvaro Esquivel RomeroNo ratings yet
- Choi 2019 Progress in OrthoDocument8 pagesChoi 2019 Progress in OrthoRohan BhagatNo ratings yet
- s40634 021 00334 1Document6 pagess40634 021 00334 1Saffa AzharaaniNo ratings yet
- Treatment Strategyfor Irreparable Rotator Cuff TearsDocument16 pagesTreatment Strategyfor Irreparable Rotator Cuff TearshawkjohnNo ratings yet
- "ACL Surgery: When To Do It?": Volker Musahl Theresa Diermeier Darren de SA Jon KarlssonDocument4 pages"ACL Surgery: When To Do It?": Volker Musahl Theresa Diermeier Darren de SA Jon Karlssonfebyan yohanesNo ratings yet
- Homemade Pin-Hook For Surgical Treatment of Posterior Cruciate Ligament Avulsion FracturesDocument7 pagesHomemade Pin-Hook For Surgical Treatment of Posterior Cruciate Ligament Avulsion Fracturesdrbane123No ratings yet
- Application - of - Nano-Carbon - and 2Document8 pagesApplication - of - Nano-Carbon - and 2andika rafaelNo ratings yet
- Periodontology 2000 - 2023 - Urban 2Document19 pagesPeriodontology 2000 - 2023 - Urban 2Spotify GuillemNo ratings yet
- Case Series of All-Arthroscopic Treatment For Terrible Triad of The Elbow: Indications and Clinical OutcomesDocument10 pagesCase Series of All-Arthroscopic Treatment For Terrible Triad of The Elbow: Indications and Clinical OutcomesdorfynatorNo ratings yet
- Skeletal Stability After 2-Jaw Surgery Via Surgery-First Approach in Facial Asymmetry Patients Using CBCTDocument8 pagesSkeletal Stability After 2-Jaw Surgery Via Surgery-First Approach in Facial Asymmetry Patients Using CBCTPhachara SiripraphonrojNo ratings yet
- Osteoarthritis and Osteoporosis 2Document38 pagesOsteoarthritis and Osteoporosis 2tarikeopsNo ratings yet
- Total Knee Replacement (TKR) Techniques: April 2019Document14 pagesTotal Knee Replacement (TKR) Techniques: April 2019NandaChintiaNo ratings yet
- Component Placement Accuracy in Unicompartmental KneeDocument3 pagesComponent Placement Accuracy in Unicompartmental Kneeswastik baratNo ratings yet
- Anterior Cruciate Ligament (ACL) Injuries A Review On The Newest Reconstruction TechniquesDocument5 pagesAnterior Cruciate Ligament (ACL) Injuries A Review On The Newest Reconstruction TechniquesAnggia PNo ratings yet
- Robotic Mechanical Alignment Vs Robotic Functional AlignmentDocument10 pagesRobotic Mechanical Alignment Vs Robotic Functional AlignmentMohan DesaiNo ratings yet
- Clinical StudyDocument13 pagesClinical StudyJuliana Gomes BarretoNo ratings yet
- Yau Et Al 2022 Swelling Assessment After Total Knee ArthroplastyDocument10 pagesYau Et Al 2022 Swelling Assessment After Total Knee ArthroplastyCláudia SilvaNo ratings yet
- EgyptOrthopJ50145-8454425 232904tgtDocument6 pagesEgyptOrthopJ50145-8454425 232904tgtAzmi FarhadiNo ratings yet
- Acetabular Reconstruction in Total Hip Arthroplasty: EditorialDocument14 pagesAcetabular Reconstruction in Total Hip Arthroplasty: Editorialana starcevicNo ratings yet
- Marcheggianimuccioli 2019Document12 pagesMarcheggianimuccioli 2019Ghusun MadaniNo ratings yet
- Proyeccion Hombro BenageaunDocument3 pagesProyeccion Hombro Benageaunherytz martinez gomezNo ratings yet
- An Acetabular Fracture With A Series of Complications and Their Solutions A Notable Case ReportDocument6 pagesAn Acetabular Fracture With A Series of Complications and Their Solutions A Notable Case ReportAthenaeum Scientific PublishersNo ratings yet
- Liu 2015Document4 pagesLiu 2015Alberto AlexandruNo ratings yet
- Mischinger2020 Article TheCriticalViewOfSafetyCVSCann PDFDocument7 pagesMischinger2020 Article TheCriticalViewOfSafetyCVSCann PDFBolivar IseaNo ratings yet
- Progressive Early Passive and Active Exercise Therapy After Surgical Rotator Cuff Repair - Study Protocol For A Randomized Controlled Trial (The CUT-N-MOVE Trial)Document12 pagesProgressive Early Passive and Active Exercise Therapy After Surgical Rotator Cuff Repair - Study Protocol For A Randomized Controlled Trial (The CUT-N-MOVE Trial)Luna Tatiana Garces DuranNo ratings yet
- Adler 2007Document11 pagesAdler 2007Anand KarnawatNo ratings yet
- Functional and Cosmetic Outcome After Reconstruction of Isolated, Unilateral Orbital Floor Fractures (Blow-Out Fractures) With and Without The Support of 3D-PrintedDocument12 pagesFunctional and Cosmetic Outcome After Reconstruction of Isolated, Unilateral Orbital Floor Fractures (Blow-Out Fractures) With and Without The Support of 3D-PrintedDoruk OrgunNo ratings yet
- Aps 39 345Document9 pagesAps 39 345isabelNo ratings yet
- 10.1186@s12903 019 0941 ZDocument18 pages10.1186@s12903 019 0941 ZJosé Carlos Herrera IbarraNo ratings yet
- Comparison of Total Patellectomy and Osteosynthesis With Tension Band WiringDocument11 pagesComparison of Total Patellectomy and Osteosynthesis With Tension Band WiringAldrovando JrNo ratings yet
- Horizontal Alveolar Ridge Augmentation in Implant Dentistry: A Surgical ManualFrom EverandHorizontal Alveolar Ridge Augmentation in Implant Dentistry: A Surgical ManualRating: 4.5 out of 5 stars4.5/5 (2)
- Comparison of 3D C-Arm Fluoroscopy and 3D Image-GuidedDocument8 pagesComparison of 3D C-Arm Fluoroscopy and 3D Image-Guidedgevowo3277No ratings yet
- s13018 018 0814 1Document9 pagess13018 018 0814 1Someshwar GuptNo ratings yet
- Materials and Techniques For Anterior Cruciate Ligament RepairDocument8 pagesMaterials and Techniques For Anterior Cruciate Ligament Repairapi-284277228No ratings yet
- Double-Row, Transosseous-Equivalent Suture-Bridge Repair For Supraspinatus Tears - Power Up The HealingDocument9 pagesDouble-Row, Transosseous-Equivalent Suture-Bridge Repair For Supraspinatus Tears - Power Up The HealingEllan Giulianno FerreiraNo ratings yet
- Intraoperative Imaging in Orbital Reconstruction: How Does It Affect The Position of The Implant?"Document6 pagesIntraoperative Imaging in Orbital Reconstruction: How Does It Affect The Position of The Implant?"quetmauhamNo ratings yet
- Short Vs Long in Osteoporotic FRDocument7 pagesShort Vs Long in Osteoporotic FRandy ardiansyahNo ratings yet
- Hook Plate With or Without CoracoclavicularDocument6 pagesHook Plate With or Without Coracoclavicularmex487No ratings yet
- Biomechanical Comparison of Anterior Cruciate Ligament Reconstruction Fixation Methods and Implications On Clinical OutcomesDocument13 pagesBiomechanical Comparison of Anterior Cruciate Ligament Reconstruction Fixation Methods and Implications On Clinical Outcomesorthotraumato30No ratings yet
- SH 3Document8 pagesSH 3ع الNo ratings yet
- Zygomatic Implants PDFDocument18 pagesZygomatic Implants PDFgirl33No ratings yet
- Meniscus Root Repair Vs Meniscectomy orDocument8 pagesMeniscus Root Repair Vs Meniscectomy orJulio Cesar Guillen MoralesNo ratings yet
- Lenny Niehaus - Jazz Conception For Saxophone Vol.1 - BasicDocument28 pagesLenny Niehaus - Jazz Conception For Saxophone Vol.1 - BasicRodrigo TaramascoNo ratings yet
- Consenso MeniscoDocument11 pagesConsenso MeniscoJulio Cesar Guillen MoralesNo ratings yet
- Menisco Current ConceptDocument7 pagesMenisco Current ConceptJulio Cesar Guillen MoralesNo ratings yet
- Billies Bounce EbDocument2 pagesBillies Bounce EbJulio Cesar Guillen MoralesNo ratings yet
- Pelvic Fractures. Part 2. Contemporary Indications and Techniques For Definitive Surgical Management PDFDocument11 pagesPelvic Fractures. Part 2. Contemporary Indications and Techniques For Definitive Surgical Management PDFJulio Cesar Guillen MoralesNo ratings yet
- Langford 2013Document10 pagesLangford 2013RezaDianPratamaNo ratings yet
- 10.1097@00124635 199605000 00004 PDFDocument9 pages10.1097@00124635 199605000 00004 PDFJulio Cesar Guillen MoralesNo ratings yet
- Pelvic Fractures. Part 2. Contemporary Indications and Techniques For Definitive Surgical Management PDFDocument11 pagesPelvic Fractures. Part 2. Contemporary Indications and Techniques For Definitive Surgical Management PDFJulio Cesar Guillen MoralesNo ratings yet
- Langford 2013Document10 pagesLangford 2013RezaDianPratamaNo ratings yet
- Inestabilidad de HombroDocument14 pagesInestabilidad de HombroJulio Cesar Guillen MoralesNo ratings yet
- Langford 2013Document10 pagesLangford 2013RezaDianPratamaNo ratings yet
- Fractura e FalangsDocument16 pagesFractura e FalangsJulio Cesar Guillen MoralesNo ratings yet
- Pie Zambo ManejoDocument74 pagesPie Zambo ManejoJulio Cesar Guillen MoralesNo ratings yet
- Hallux RigidusDocument66 pagesHallux RigidusJulio Cesar Guillen Morales100% (1)
- Eric Marienthal Book For AppDocument47 pagesEric Marienthal Book For AppAlex Ensing96% (24)
- Ankle Ligaments On MRI: Appearance of Normal and Injured LigamentsDocument9 pagesAnkle Ligaments On MRI: Appearance of Normal and Injured Ligamentspjanu86No ratings yet
- The Epidemiology of Needle Stick Injuries AmongDocument8 pagesThe Epidemiology of Needle Stick Injuries AmongJulio Cesar Guillen MoralesNo ratings yet
- Programme: P D C DDocument6 pagesProgramme: P D C DJulio Cesar Guillen MoralesNo ratings yet
- Eric Marienthal - The Two Hour Practice Session PDFDocument12 pagesEric Marienthal - The Two Hour Practice Session PDFNtersblich94% (18)
- Clinical Results With The Medennium Phakic Refractive Lens For The Correction of High MyopiaDocument1 pageClinical Results With The Medennium Phakic Refractive Lens For The Correction of High MyopiaJulio Cesar Guillen MoralesNo ratings yet
- Abstracts of The CongreoDocument35 pagesAbstracts of The CongreoJulio Cesar Guillen MoralesNo ratings yet
- Moth Balls: Safety Data SheetDocument9 pagesMoth Balls: Safety Data SheethafilrediandikaNo ratings yet
- PuppetryDocument183 pagesPuppetryÉva Hegedüsné50% (2)
- BioassayDocument38 pagesBioassayMuhammad Masoom AkhtarNo ratings yet
- MAPEH Activity Sheet Q2-Week1Document7 pagesMAPEH Activity Sheet Q2-Week1John King johnking.monderinNo ratings yet
- Isu Dan Etika Pada Perawatan Paliatif PDFDocument17 pagesIsu Dan Etika Pada Perawatan Paliatif PDFNatasya ChieCaem FunforeverNo ratings yet
- Valid RRR Application 2013 - 2017 PDFDocument22,467 pagesValid RRR Application 2013 - 2017 PDFAyub NaveedNo ratings yet
- Ims 1 10 18Document2 pagesIms 1 10 18Katherine UrregoNo ratings yet
- Art Comparison Essay ExampleDocument5 pagesArt Comparison Essay Exampleflrzcpaeg100% (2)
- The Effectiveness of Treatment For Sexual Offenders PDFDocument30 pagesThe Effectiveness of Treatment For Sexual Offenders PDFBlack magikNo ratings yet
- Eritro Papulo Skuamosa 2021Document47 pagesEritro Papulo Skuamosa 2021Yolanda Agnesia Purba0% (1)
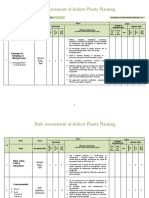
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet
- Second Circuit Public Charge RulingDocument110 pagesSecond Circuit Public Charge RulingLaw&CrimeNo ratings yet
- Wipe Sampling Materials For Lead in Surface DustDocument3 pagesWipe Sampling Materials For Lead in Surface DustAhmad Zubair RasulyNo ratings yet
- Dheeraj DumirDocument11 pagesDheeraj DumirAnonymous CR8v7xb0No ratings yet
- Influence of Potassium Sulfate On Faba Bean Yield and QualityDocument9 pagesInfluence of Potassium Sulfate On Faba Bean Yield and QualityMoehammad AlqamariNo ratings yet
- Short StoryDocument5 pagesShort Storyapi-376081909No ratings yet
- Earth Fare PresentationDocument36 pagesEarth Fare Presentationapi-253275458No ratings yet
- MSPE Noteworthy Characteristics Worksheet: Complete This Worksheet and Bring It To Your Mandatory Career Advising SessionDocument2 pagesMSPE Noteworthy Characteristics Worksheet: Complete This Worksheet and Bring It To Your Mandatory Career Advising SessionHải Dương NguyễnNo ratings yet
- Nursing Care Plan For Patients With FractureDocument3 pagesNursing Care Plan For Patients With Fracture_cezca_89% (168)
- Nepal New Emerging Pharma MarketDocument5 pagesNepal New Emerging Pharma MarketDeep_HeartNo ratings yet
- 02 2020 Tuaha Adil and Dr. Faisal JamilDocument39 pages02 2020 Tuaha Adil and Dr. Faisal JamilKhadijaNo ratings yet
- CXC Csec English A June 2015 p1Document16 pagesCXC Csec English A June 2015 p1Rihanna Johnson100% (1)
- ECGforinternsDocument25 pagesECGforinternsusmleusmle86No ratings yet
- Understanding Violence-Does Psychoanalytic Thinking matter-J.Yakeley&J.R.Meloy PDFDocument11 pagesUnderstanding Violence-Does Psychoanalytic Thinking matter-J.Yakeley&J.R.Meloy PDFMihaela BalionNo ratings yet
- SITHKOP005 - Written AssessmentDocument7 pagesSITHKOP005 - Written AssessmentTephieNo ratings yet
- The Peat WhispererDocument85 pagesThe Peat Whispererzarrin77100% (6)
- (S. Abbate) Ear Acupuncture Prescriptions and Techniques PDFDocument8 pages(S. Abbate) Ear Acupuncture Prescriptions and Techniques PDFVenom VerdinNo ratings yet
- GWC - Company ProfileDocument4 pagesGWC - Company Profileelrajil100% (1)
- HSE National Cleaning Standards ManualDocument149 pagesHSE National Cleaning Standards ManualNemer MansourNo ratings yet
- Global Poverty PowerPointDocument15 pagesGlobal Poverty PowerPointАдылхан БаймуратовNo ratings yet