You might also like
- Organs in The Body Quadrants and RegionsDocument3 pagesOrgans in The Body Quadrants and RegionsDavid HosamNo ratings yet
- Ashtma Timeline T2Document21 pagesAshtma Timeline T2ISABEL SOFIA CABARCAS COGOLLONo ratings yet
- Allergic BronchitisDocument18 pagesAllergic BronchitisTeresa EvansNo ratings yet
- Bubi EstDocument13 pagesBubi EstandrikeishaNo ratings yet
- W1 L4 Asthma in ChildrenDocument61 pagesW1 L4 Asthma in ChildrenAnas FikriNo ratings yet
- New Insights Into The Relationship Between Airway Inflammation and AsthmaDocument11 pagesNew Insights Into The Relationship Between Airway Inflammation and Asthmaapi-3736350No ratings yet
- BCP 0372 PDFDocument8 pagesBCP 0372 PDFPoetri LaelahNo ratings yet
- Chapter 9. Bronchial Asthma: Khaled O Hadeli MD, FCCPDocument19 pagesChapter 9. Bronchial Asthma: Khaled O Hadeli MD, FCCPgireeshsachinNo ratings yet
- Proceedings: 1120 of The Royal Society of Medicine 36Document7 pagesProceedings: 1120 of The Royal Society of Medicine 36fiji drNo ratings yet
- Asthama - Pathology and PathophysiologyDocument5 pagesAsthama - Pathology and PathophysiologyTejal ParulkarNo ratings yet
- Asthma: Allergy Asthma and Clinical Immunology November 2011Document10 pagesAsthma: Allergy Asthma and Clinical Immunology November 2011Sarmad AlwardiNo ratings yet
- 132184-Article Text-356446-1-10-20160317Document7 pages132184-Article Text-356446-1-10-20160317aslamNo ratings yet
- Pathogenic Mechanisms in Asthma and COPDDocument24 pagesPathogenic Mechanisms in Asthma and COPDWilliamRayCassidyNo ratings yet
- The History of COPDDocument12 pagesThe History of COPDcarloscano1994No ratings yet
- 1 s2.0 S0304416511001358 MainDocument8 pages1 s2.0 S0304416511001358 MainjackashcaNo ratings yet
- Asthma Patofisiologi 1Document8 pagesAsthma Patofisiologi 1Maulana Aufar Firwanda DriveNo ratings yet
- J1-T4 CorticosteroidsDocument11 pagesJ1-T4 CorticosteroidsGoblin HunterNo ratings yet
- NIH Public Access: Author ManuscriptDocument18 pagesNIH Public Access: Author Manuscriptmaria martinezNo ratings yet
- Ajprm v9 Id1085Document8 pagesAjprm v9 Id1085Maira IrshadNo ratings yet
- BarnesnriDocument11 pagesBarnesnriAndry Wahyudi AgusNo ratings yet
- Asthma Phenotypes PDFDocument10 pagesAsthma Phenotypes PDFPhuong HuynhNo ratings yet
- Asthma 2Document8 pagesAsthma 2Evangelist Stephen NziokaNo ratings yet
- Im B4.9 CopdDocument9 pagesIm B4.9 CopdCC Samson, Caesar AnthonyNo ratings yet
- Immunology of Asthma and Chronic Obstructive Pulmonary DiseaseDocument10 pagesImmunology of Asthma and Chronic Obstructive Pulmonary DiseaseClaudio Luis VenturiniNo ratings yet
- Bronchial AsthmaDocument7 pagesBronchial AsthmaAparajitaNo ratings yet
- Asma Exacerbacioes EpidemiologiaDocument7 pagesAsma Exacerbacioes Epidemiologiahebert ramosNo ratings yet
- From The Department of Physiology, Harvard School of Public Health, Boston, MassDocument16 pagesFrom The Department of Physiology, Harvard School of Public Health, Boston, MasshyperbarichealthNo ratings yet
- Asthma Thesis StatementDocument4 pagesAsthma Thesis Statementfjnev0hc100% (2)
- Physical Therapy For Children With ChronDocument11 pagesPhysical Therapy For Children With ChronGauravNo ratings yet
- Bronchial Asthma Research PaperDocument6 pagesBronchial Asthma Research Paperniisexgkf100% (1)
- Immunology of Asthma and ChronicDocument10 pagesImmunology of Asthma and ChronicMeldaNo ratings yet
- A Bronchographic Sign of Chronic: Bronchitis'Document4 pagesA Bronchographic Sign of Chronic: Bronchitis'Ziyan NafisahNo ratings yet
- Inmunologia Asma y EpocDocument10 pagesInmunologia Asma y EpocAnailil MoralesNo ratings yet
- Bates 2009 Modelos Animales de AsmaDocument11 pagesBates 2009 Modelos Animales de Asmalucia coronaNo ratings yet
- Pa Tho Physiology of AsthmaDocument18 pagesPa Tho Physiology of AsthmaNeil-Vince ConejosNo ratings yet
- Bronchial AsthmaDocument34 pagesBronchial AsthmaFabb NelsonNo ratings yet
- Pathophysiological Mechanisms of Asthma: Andrew BushDocument17 pagesPathophysiological Mechanisms of Asthma: Andrew BushDianNo ratings yet
- Cellular and Molecular Mechanisms of Asthma and COPDDocument18 pagesCellular and Molecular Mechanisms of Asthma and COPDMihaela BerindeieNo ratings yet
- Asthma Phenotypes The Evolution From Clinical To MDocument11 pagesAsthma Phenotypes The Evolution From Clinical To MNóra FerenczyNo ratings yet
- Anti Interleukin PDFDocument4 pagesAnti Interleukin PDFPaulita LafauxNo ratings yet
- Ats 2022Document10 pagesAts 2022EN BUNo ratings yet
- Asthma: Practice EssentialsDocument12 pagesAsthma: Practice EssentialsIda WilonaNo ratings yet
- Definisi AsmaDocument12 pagesDefinisi AsmaDayu Punik ApsariNo ratings yet
- Eustis Toxins and Asthma 4 1912Document4 pagesEustis Toxins and Asthma 4 1912IGNo ratings yet
- Asma en El AncianoDocument5 pagesAsma en El AncianoSara PérezNo ratings yet
- Asthma: Whom Does It Affect?Document11 pagesAsthma: Whom Does It Affect?Ken KennyNo ratings yet
- 1924426Document4 pages1924426Langat IsaacNo ratings yet
- Chest Radiography Radiographers: An Introduction To For StudentDocument29 pagesChest Radiography Radiographers: An Introduction To For StudentDragan YottNo ratings yet
- Oxygen Toxicity: Maj Anuj Chawla Col Ak LavaniaDocument3 pagesOxygen Toxicity: Maj Anuj Chawla Col Ak LavanianiarNo ratings yet
- 242 FullDocument3 pages242 FullJosh SeeleyNo ratings yet
- Bronchodilation Effects of Kalachuchi Leaves (Plumeria Induced BronchoconstrictionDocument15 pagesBronchodilation Effects of Kalachuchi Leaves (Plumeria Induced BronchoconstrictionLenny Mae JagosNo ratings yet
- Pone 0062827Document12 pagesPone 0062827Tiffany NurzamanNo ratings yet
- Asthma Mechanisms: Key PointsDocument6 pagesAsthma Mechanisms: Key PointsAfrian RahmandaNo ratings yet
- Pathophysiology of AsthmaDocument71 pagesPathophysiology of AsthmaChin ChanNo ratings yet
- Introduction: The Artificial Lung Collapse of Forlanini: Go ToDocument3 pagesIntroduction: The Artificial Lung Collapse of Forlanini: Go ToniqqazNo ratings yet
- Fast Facts: Asthma: Improve patient self-management and drug use, achieve asthma controlFrom EverandFast Facts: Asthma: Improve patient self-management and drug use, achieve asthma controlNo ratings yet
- Childhood Asthma: DR - Rodman Tarigan, Spa.,MkesDocument35 pagesChildhood Asthma: DR - Rodman Tarigan, Spa.,MkesBambang IrwansyahNo ratings yet
- Asthma Research Paper OutlineDocument8 pagesAsthma Research Paper Outlineaflbsybmc100% (1)
- Oxygen ToxicityDocument4 pagesOxygen ToxicityRicard ClainkweeNo ratings yet
- Assissment Form FixDocument8 pagesAssissment Form FixUlfatun ChasanahNo ratings yet
- HypothalamusDocument38 pagesHypothalamuscmabdullahNo ratings yet
- To Receive Daily FREE GK, Exams SMS Alerts, Sms JOIN RADIANTNPSC To 09870807070Document5 pagesTo Receive Daily FREE GK, Exams SMS Alerts, Sms JOIN RADIANTNPSC To 09870807070Aruna AzhagarasanNo ratings yet
- Summative Test - Biotech2022Document6 pagesSummative Test - Biotech2022Joan VillarcaNo ratings yet
- Cell Transport MechanismsDocument21 pagesCell Transport MechanismsCj CasintoNo ratings yet
- E Book L PRF e Stick Bone - Passei Direto9 PDFDocument1 pageE Book L PRF e Stick Bone - Passei Direto9 PDFRENATO SUDATINo ratings yet
- Kine 2p90 l17Document7 pagesKine 2p90 l17baileyschaefer28No ratings yet
- Assesing A Casualty Vital SignsDocument19 pagesAssesing A Casualty Vital SignsCiedelle Honey Lou DimaligNo ratings yet
- Vetsci 10 00160Document20 pagesVetsci 10 00160Ana Paula De Souza LimaNo ratings yet
- Acute Atrial Fibrillation DavidsonDocument6 pagesAcute Atrial Fibrillation DavidsonAamir BugtiNo ratings yet
- Du 24Document2 pagesDu 24BDI92No ratings yet
- DLL in GEN BIODocument14 pagesDLL in GEN BIOBernadette Jeane Aquino GarciaNo ratings yet
- Periodical TestDocument4 pagesPeriodical TestnonononowayNo ratings yet
- Juliao Gb-29: Stationary CreviceDocument1 pageJuliao Gb-29: Stationary Creviceray72roNo ratings yet
- Heat Stroke ArticleDocument29 pagesHeat Stroke ArticleIurascu GeaninaNo ratings yet
- Kundalini Yoga - Exercise Set For Maintaining A Flexible Spine.Document8 pagesKundalini Yoga - Exercise Set For Maintaining A Flexible Spine.mybestself100% (3)
- 36 Drying of Wood Principles and PracticesDocument59 pages36 Drying of Wood Principles and PracticesHugodezanNo ratings yet
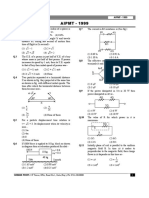
- Aipmt 1999Document16 pagesAipmt 1999sumit kumarNo ratings yet
- Cardiac Tamponade and ManagementDocument42 pagesCardiac Tamponade and ManagementRezwanul Hoque Bulbul100% (2)
- The Eightextraordinary VesselsDocument9 pagesThe Eightextraordinary Vesselsrubenildo_coutinhoNo ratings yet
- HCG Stimulation TestDocument3 pagesHCG Stimulation Testsanham100% (1)
- Introduction To BiomaterialsDocument74 pagesIntroduction To Biomaterialspayaliya91No ratings yet
- Yeast in Batch Culture - Expt - 4 - Shake Flask - Part 1 - 4th EdDocument7 pagesYeast in Batch Culture - Expt - 4 - Shake Flask - Part 1 - 4th EdRachel HechanovaNo ratings yet
- AlkaloidsDocument44 pagesAlkaloidssangram_pharma9145100% (2)
- Bioavailability: How The Nutrients in Food Become Available To Our BodiesDocument2 pagesBioavailability: How The Nutrients in Food Become Available To Our BodiesTheAwein ChannelNo ratings yet
- The Urinary SystemDocument46 pagesThe Urinary SystemWeb AredomNo ratings yet
- Example 1.5 - 1.8 Modeling Binary DataDocument20 pagesExample 1.5 - 1.8 Modeling Binary DataLidia MayangsariNo ratings yet
- Ijspt 10 760 PDFDocument27 pagesIjspt 10 760 PDFMustafid Alwi AlvaroNo ratings yet
- Yogoda 1st EditionDocument29 pagesYogoda 1st EditionChadalavada Venkata Sai Pradeep100% (5)
- UTIDocument53 pagesUTIMimi Suhaini SudinNo ratings yet