You might also like
- ServSafe 7th Edition Full PDFDocument366 pagesServSafe 7th Edition Full PDFAissie Tribiana90% (49)
- Nutrients A-Z (gnv64) PDFDocument354 pagesNutrients A-Z (gnv64) PDFAnil Penumacha100% (1)
- Parasites and Allergy, 2006 PDFDocument215 pagesParasites and Allergy, 2006 PDFtrubus100% (1)
- Pulmonary Tuberculosis: Presented By: Mis.M.K.Kaku Nursing TutorDocument16 pagesPulmonary Tuberculosis: Presented By: Mis.M.K.Kaku Nursing TutorKaku ManishaNo ratings yet
- Ischemic Heart DiseaseDocument116 pagesIschemic Heart DiseaseAndrew OrlovNo ratings yet
- Gastro Tract InfectionsDocument69 pagesGastro Tract Infectionsmagi_No ratings yet
- United States District Court Middle District of Florida Orlando DivisionDocument12 pagesUnited States District Court Middle District of Florida Orlando DivisionJ Rohrlich100% (1)
- AsthmaDocument46 pagesAsthmaHafiz Muhammad AeymonNo ratings yet
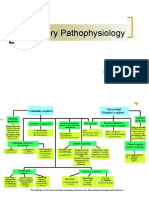
- Respiratory Pathophysiology: B. Pimentel, M.D. University of Makati College of NursingDocument12 pagesRespiratory Pathophysiology: B. Pimentel, M.D. University of Makati College of NursingDoc JacqueNo ratings yet
- OrganophosphateDocument21 pagesOrganophosphatehendra_darmawan_4No ratings yet
- Bronchial AsthmaDocument46 pagesBronchial AsthmaKhor Kee GuanNo ratings yet
- Anal FistulaDocument26 pagesAnal FistulaBeverly PagcaliwaganNo ratings yet
- Pulmonaryembolism 150329161109 Conversion Gate01Document60 pagesPulmonaryembolism 150329161109 Conversion Gate01Rafika RaraNo ratings yet
- Cardiovascular System: by DR - Nuha Abdel GhaffarDocument41 pagesCardiovascular System: by DR - Nuha Abdel GhaffarMohammed Alaa EldeanNo ratings yet
- Pathophysiology of Tuberculosis: Group 5 Latosa, Selene Lee, Guk Lim, Johanna Magalona, Stephen Mendoza, ColeenDocument22 pagesPathophysiology of Tuberculosis: Group 5 Latosa, Selene Lee, Guk Lim, Johanna Magalona, Stephen Mendoza, ColeenAlexander Santiago ParelNo ratings yet
- Asthma: Rochelle M. Nolte, MD CDR Usphs Family MedicineDocument56 pagesAsthma: Rochelle M. Nolte, MD CDR Usphs Family MedicineJoan Marie Lechado InoviaNo ratings yet
- Diagnosis & Treament: ShockDocument52 pagesDiagnosis & Treament: ShockasepNo ratings yet
- 16 Martie - Curs BPOC - SlideDocument95 pages16 Martie - Curs BPOC - Slidejonah1024No ratings yet
- Acute Respiratory Distress Syndrome (ARDS)Document72 pagesAcute Respiratory Distress Syndrome (ARDS)desyNo ratings yet
- Asthma and CopdDocument44 pagesAsthma and CopdBeer Dilacshe100% (1)
- Viral Exanthem (Main)Document94 pagesViral Exanthem (Main)Starlet Rhonadez Bito-onon OrielNo ratings yet
- Tuberculosis: Communicable DiseaseDocument6 pagesTuberculosis: Communicable DiseaseMiguel Cuevas DolotNo ratings yet
- Bronchial AsthmaDocument39 pagesBronchial AsthmaSaeed mohamed100% (1)
- Asthma: Pio T. Esguerra II, MD, FPCP, FPCCP Pulmonary & Critical Care FEU-NRMF Medical CenterDocument98 pagesAsthma: Pio T. Esguerra II, MD, FPCP, FPCCP Pulmonary & Critical Care FEU-NRMF Medical CenteryayayanizaNo ratings yet
- CACCN Certification Study Guide Questions Mar 2010Document27 pagesCACCN Certification Study Guide Questions Mar 2010BrittBrattDubb100% (1)
- Bronchiectasis: By: Karunesh KumarDocument21 pagesBronchiectasis: By: Karunesh KumarAnkan DeyNo ratings yet
- Dyspnea PresentationDocument37 pagesDyspnea PresentationamgoperaNo ratings yet
- Bronchial AsthmaDocument45 pagesBronchial Asthmamuluken mulatieNo ratings yet
- Aria Guidelines 2020Document14 pagesAria Guidelines 2020xtine100% (2)
- Bronchiectasis: Prepared By: Michelle TamorDocument17 pagesBronchiectasis: Prepared By: Michelle TamorMichelle TamorNo ratings yet
- EpistaxisDocument33 pagesEpistaxispaulyn ramosNo ratings yet
- Module 5A: Dental Management of Patients With Asthma: Prepared By: Dr. Maria Luisa Ramos - ClementeDocument27 pagesModule 5A: Dental Management of Patients With Asthma: Prepared By: Dr. Maria Luisa Ramos - Clementeelaine100% (1)
- Bronchiectasis NishaDocument44 pagesBronchiectasis NishaKaarthigan RamaiahNo ratings yet
- Case Discussion - CopdDocument63 pagesCase Discussion - CopdrajeshNo ratings yet
- Hydrocarbon PoisoningDocument10 pagesHydrocarbon PoisoningVarshith GandlaNo ratings yet
- Rheumatic Fever: DR: Kaem Shir AliDocument24 pagesRheumatic Fever: DR: Kaem Shir AliMwanja Moses100% (1)
- 02 Bronchial Asthma Circ 2018-2019Document15 pages02 Bronchial Asthma Circ 2018-2019Mooha Alanzy100% (1)
- Lower Respiratory Tract InfectionDocument9 pagesLower Respiratory Tract InfectionNamrah AfzalNo ratings yet
- Respiration 16 Respiratory FailureDocument31 pagesRespiration 16 Respiratory Failureapi-19641337No ratings yet
- CopdDocument14 pagesCopdMohd Farid Bin RosliNo ratings yet
- Asthma Management and Prevention in ChildrenDocument57 pagesAsthma Management and Prevention in ChildrenSundararajaperumal AnandhakrishnanNo ratings yet
- Miliary TB NewDocument23 pagesMiliary TB Newzakariah kamalNo ratings yet
- Acute Respiratory Distress SyndromDocument38 pagesAcute Respiratory Distress SyndrompatriaindraNo ratings yet
- Bronchial AsthmaDocument20 pagesBronchial AsthmaJuliet De GuzmanNo ratings yet
- Onchial AsthmaDocument13 pagesOnchial Asthmaram krishna100% (1)
- Endotracheal TubeDocument14 pagesEndotracheal TubeValerie BlasNo ratings yet
- Cough: PHR Sangita ShakyaDocument21 pagesCough: PHR Sangita ShakyaCurex QANo ratings yet
- Lung Abscess: Dr. Ravi Gadani MS, FmasDocument20 pagesLung Abscess: Dr. Ravi Gadani MS, FmasRaviNo ratings yet
- Bronchial Asthma (1) SKDocument24 pagesBronchial Asthma (1) SKSafoora RafeeqNo ratings yet
- Isabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderDocument15 pagesIsabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderCharlz ZipaganNo ratings yet
- Drugs Acting On Functions of Respiratory SystemDocument73 pagesDrugs Acting On Functions of Respiratory SystemMarin ChianuNo ratings yet
- PT Case: Copd Exacerbation: DedicationDocument10 pagesPT Case: Copd Exacerbation: DedicationDianaLopezBorjaNo ratings yet
- Copd Omc Class - BB PDFDocument29 pagesCopd Omc Class - BB PDFafaq alismailiNo ratings yet
- Respiratory EmergenciesDocument34 pagesRespiratory EmergenciesRoshana MallawaarachchiNo ratings yet
- Bronchial AsthmaDocument11 pagesBronchial AsthmaFaria Islam JuhiNo ratings yet
- Emphysema Case Study AnalysisDocument10 pagesEmphysema Case Study AnalysisEfren VisteNo ratings yet
- Lung Abscess Bronchoectasis PleurisynDocument19 pagesLung Abscess Bronchoectasis Pleurisynmarco luenaNo ratings yet
- Acute Respiratory Distress SyndromeDocument10 pagesAcute Respiratory Distress Syndromealina abu rumiNo ratings yet
- Case AppendicitisDocument30 pagesCase AppendicitisSarahNo ratings yet
- Oxygen TherapyDocument31 pagesOxygen TherapyChayan BhowmikNo ratings yet
- SHOCKDocument35 pagesSHOCKsami azadNo ratings yet
- Exudative Pleural Effusions - UpToDateDocument2 pagesExudative Pleural Effusions - UpToDateAsif IqbalNo ratings yet
- CopdDocument74 pagesCopdSardor AnorboevNo ratings yet
- AsthmaDocument6 pagesAsthmaJay Hipulan QuiranteNo ratings yet
- AsthmaDocument5 pagesAsthmaabenezer isayasNo ratings yet
- Peanuts As Functional Food: A ReviewDocument28 pagesPeanuts As Functional Food: A ReviewLPATI12No ratings yet
- Allergy 2010Document7 pagesAllergy 2010HAOMSNo ratings yet
- Bronchial Asthma!: A C E S G V CDocument10 pagesBronchial Asthma!: A C E S G V CAmalNo ratings yet
- BilastineDocument1 pageBilastineCharess Candelon - SengcoNo ratings yet
- Universiti Teknologi MaraDocument38 pagesUniversiti Teknologi MaraFitriy ElmyNo ratings yet
- Primary School Menu April - October 2016Document8 pagesPrimary School Menu April - October 2016Vicky McLachlanNo ratings yet
- (Osborn) Chapter 60: Learning Outcome 1 Learning Outcome 2 Learning Outcome 3Document14 pages(Osborn) Chapter 60: Learning Outcome 1 Learning Outcome 2 Learning Outcome 3KittiesNo ratings yet
- Section 3 Reading Comprehension Time: 55 MinutesDocument6 pagesSection 3 Reading Comprehension Time: 55 MinutesFe Fe100% (1)
- Implication of Allergy and Atopy in IgG4 Related DDocument18 pagesImplication of Allergy and Atopy in IgG4 Related DjosehannaNo ratings yet
- Medical Devices Manufactured From Latex: European Regulatory InitiativesDocument6 pagesMedical Devices Manufactured From Latex: European Regulatory InitiativesAdel AdielaNo ratings yet
- Fragrances and EoDocument24 pagesFragrances and EoioanaNo ratings yet
- Guidelines For The Management of Latex Allergies A PDFDocument23 pagesGuidelines For The Management of Latex Allergies A PDFmilenaicaNo ratings yet
- 1994 - André Et Al. - Role of New Allergens and of Allergens Consumption in The Increased Incidence of Food Sensitizations in FranceDocument7 pages1994 - André Et Al. - Role of New Allergens and of Allergens Consumption in The Increased Incidence of Food Sensitizations in FrancePJ Chalet BookNo ratings yet
- QuizDocument7 pagesQuizapi-233757196No ratings yet
- Mycoprotein ProductionDocument10 pagesMycoprotein ProductionBabuskin SrinivasanNo ratings yet
- HypersensitivityDocument15 pagesHypersensitivityTejpalNo ratings yet
- Food Allergy TrainingDocument10 pagesFood Allergy TrainingHakim AliNo ratings yet
- Hypersensitivity Rev BWDocument34 pagesHypersensitivity Rev BWGuhanNo ratings yet
- Allergy Immunotherapy The Future of Allergy TreatmDocument13 pagesAllergy Immunotherapy The Future of Allergy TreatmEverton MonteiroNo ratings yet
- Managing Food Allergen Information: Safe MethodDocument2 pagesManaging Food Allergen Information: Safe MethodAlghubariNo ratings yet
- L3 - Bronchial AsthmaDocument37 pagesL3 - Bronchial Asthmazaini nieNo ratings yet
- Detecting Allergens in FoodDocument218 pagesDetecting Allergens in FoodNatassia CampbellNo ratings yet
- Alr 22073Document245 pagesAlr 22073Ummi HaniNo ratings yet
- AllergiesDocument9 pagesAllergiesClark Angelo JuanNo ratings yet
- Anaphylaxis and Epinephrine Auto-InjectorDocument7 pagesAnaphylaxis and Epinephrine Auto-Injectorqueennita69No ratings yet