You might also like
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Nursing Care of Clients Before and After CABGDocument46 pagesNursing Care of Clients Before and After CABGshejila c hNo ratings yet
- Physiology Final Exam - Glory 2017 PDFDocument14 pagesPhysiology Final Exam - Glory 2017 PDFMohammad BarakatNo ratings yet
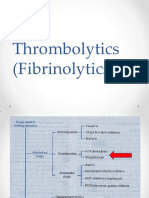
- Thrombolytics (Fibrinolytics)Document14 pagesThrombolytics (Fibrinolytics)J lodhiNo ratings yet
- Spa PPT - FinalDocument45 pagesSpa PPT - FinalShivam DwivediNo ratings yet
- Post Operative HemorrhageDocument16 pagesPost Operative Hemorrhagenishimura89No ratings yet
- Cardiology MCQDocument2 pagesCardiology MCQmohamed mowafeyNo ratings yet
- Cholinergic DrugsDocument15 pagesCholinergic DrugsChris Girgis100% (1)
- 1 - Introduction To Gastroenterology (2) SlaytDocument31 pages1 - Introduction To Gastroenterology (2) SlaytZeynep ArasNo ratings yet
- Compartment Syndrome Diagnosis and TreatmentDocument3 pagesCompartment Syndrome Diagnosis and TreatmentTantyo Adi P100% (2)
- Medical Mnemonic 1 PDFDocument3 pagesMedical Mnemonic 1 PDFJ MNo ratings yet
- Cardiovascular System: by DR - Nuha Abdel GhaffarDocument41 pagesCardiovascular System: by DR - Nuha Abdel GhaffarMohammed Alaa EldeanNo ratings yet
- HypothyroidismDocument54 pagesHypothyroidismagakshat23No ratings yet
- Orientation To Blood Bank 2Document24 pagesOrientation To Blood Bank 2Darshita SharmaNo ratings yet
- Renal Lab Tests ExplainedDocument67 pagesRenal Lab Tests ExplainedRjDNo ratings yet
- Main Applications of ECG DiagnosisDocument19 pagesMain Applications of ECG DiagnosisMaria Rowena O. SalvoNo ratings yet
- Needle Cricothyroidotomy 2 - Hatem AlsrourDocument32 pagesNeedle Cricothyroidotomy 2 - Hatem Alsrourhatem alsrour100% (2)
- CVP MonitoringDocument24 pagesCVP MonitoringChoji Heiwajima100% (1)
- 02 Bronchial Asthma Circ 2018-2019Document15 pages02 Bronchial Asthma Circ 2018-2019Mooha Alanzy100% (1)
- Pharmacology of Thyroid and Antithyroid DrugsDocument16 pagesPharmacology of Thyroid and Antithyroid DrugsVikas Viki100% (1)
- Muscle Relaxants Classification and Mechanisms of ActionDocument22 pagesMuscle Relaxants Classification and Mechanisms of Actionvinay0717100% (1)
- Nursing Assessment:: Intervention Rationale Independent InterventionsDocument2 pagesNursing Assessment:: Intervention Rationale Independent Interventionsnananana123No ratings yet
- Quiz With AnswersDocument8 pagesQuiz With Answersval284yNo ratings yet
- Git Exam 2015 PDFDocument50 pagesGit Exam 2015 PDFIbrahim BarhamNo ratings yet
- Ameliorative Efficacy of Ethanolic Extracts ofDocument13 pagesAmeliorative Efficacy of Ethanolic Extracts ofInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Colloids and CrystalooidsDocument42 pagesColloids and Crystalooidsلؤي زعيترNo ratings yet
- MCQDocument4 pagesMCQEliza SparkNo ratings yet
- Types of Shock MnemonicDocument4 pagesTypes of Shock Mnemonicrida hafeezNo ratings yet
- Congestive Cardiac Failure GuideDocument61 pagesCongestive Cardiac Failure GuideYAMINIPRIYANNo ratings yet
- Physiology Practical Measurement of Blood PressureDocument6 pagesPhysiology Practical Measurement of Blood PressureAli MohamedNo ratings yet
- Bio StatisticsDocument101 pagesBio StatisticshferdjalNo ratings yet
- Body Fluid DistributionDocument56 pagesBody Fluid DistributionZoya Morani100% (1)
- Pleural Fluid AnalysisDocument15 pagesPleural Fluid AnalysisNatalie Sarah MoonNo ratings yet
- Cardiovascular PharmacologyDocument20 pagesCardiovascular PharmacologyAliceAliceNo ratings yet
- Introduction To Cell PhysiologyDocument39 pagesIntroduction To Cell Physiologywaqas_xsNo ratings yet
- Anesthetic Consideration For Patients With Obstructive JaundiceDocument47 pagesAnesthetic Consideration For Patients With Obstructive JaundiceagatakassaNo ratings yet
- Antiadrenergic Drugs 23.07.018 PDFDocument23 pagesAntiadrenergic Drugs 23.07.018 PDFHitesh karnNo ratings yet
- Pharmacology (Intro-Drug Calculation)Document46 pagesPharmacology (Intro-Drug Calculation)May Chelle ErazoNo ratings yet
- GCNM - Lecture 1Document45 pagesGCNM - Lecture 1itsukoNo ratings yet
- Cardiac Cycle of The Heart PPT 3Document18 pagesCardiac Cycle of The Heart PPT 3pshantanu123No ratings yet
- Antituberculous Therapy in Special SituationsDocument8 pagesAntituberculous Therapy in Special SituationsMobeen Raza100% (1)
- Electrical Properties of The HeartDocument25 pagesElectrical Properties of The HeartSherwan R Shal100% (3)
- Congenital Heart DiseaseDocument45 pagesCongenital Heart DiseaseBrandedlovers OnlineshopNo ratings yet
- Ceftriaxone PDFDocument1 pageCeftriaxone PDFveniNo ratings yet
- Assessment of Urinary SystemDocument4 pagesAssessment of Urinary SystemMabesNo ratings yet
- Somatosensory System OkDocument47 pagesSomatosensory System OkIrayumastutiNo ratings yet
- Head and Neck QuestionsDocument3 pagesHead and Neck QuestionsVeriteNo ratings yet
- Antepartum Haemorrhage: BY: Ms. R. Liangkiuwiliu Assistant Professor, Obg SSNSR, SuDocument44 pagesAntepartum Haemorrhage: BY: Ms. R. Liangkiuwiliu Assistant Professor, Obg SSNSR, SuLiangkiuwiliuNo ratings yet
- PancreatitisDocument59 pagesPancreatitisAarif RanaNo ratings yet
- Hemodynamic Disorders-RevisedDocument118 pagesHemodynamic Disorders-Revisedspringding0% (1)
- MCQ Discussion SuturesDocument2 pagesMCQ Discussion SuturesHasini SamarasingheNo ratings yet
- ShockDocument21 pagesShockMin-Joo Esther ParkNo ratings yet
- Otitis Media: Dr. YasserDocument64 pagesOtitis Media: Dr. YasserYasser GaberNo ratings yet
- Cogan Syndrome Surger 4, AnkitDocument18 pagesCogan Syndrome Surger 4, AnkitAnkit Tonger AnkyNo ratings yet
- HyphemaDocument19 pagesHyphemaLiyanti RinceNo ratings yet
- BMWDocument24 pagesBMWPabhat Kumar100% (1)
- PARAQUAT POISIONING 3rd Block Imed COMPLIEDDocument15 pagesPARAQUAT POISIONING 3rd Block Imed COMPLIEDMohil PratapNo ratings yet
- Hunting Reaction - WikipediaDocument6 pagesHunting Reaction - WikipediaMashal GulNo ratings yet
- SpinalinjuryDocument29 pagesSpinalinjurymustikaNo ratings yet
- ShockDocument8 pagesShockАчпже Чпжечу100% (1)
- Dental Cements and Its Role in Crown CementationDocument30 pagesDental Cements and Its Role in Crown Cementationsami azadNo ratings yet
- CLEANING AND DISINFECTION METHOD FOR Acrylic OrthodonticsDocument23 pagesCLEANING AND DISINFECTION METHOD FOR Acrylic Orthodonticssami azadNo ratings yet
- Orofacial Soft Tissue Injury and Wound HealingDocument27 pagesOrofacial Soft Tissue Injury and Wound Healingsami azadNo ratings yet
- Etiology of MalocclusionDocument42 pagesEtiology of Malocclusionsami azadNo ratings yet
- HAEMORRHAGE CLASSIFICATION AND MANAGEMENTDocument22 pagesHAEMORRHAGE CLASSIFICATION AND MANAGEMENTsami azadNo ratings yet
- Card 1 OmsDocument15 pagesCard 1 Omssami azadNo ratings yet
- Border Moulding and Vertical Dimension ItemDocument16 pagesBorder Moulding and Vertical Dimension Itemsami azadNo ratings yet
- Antibiotic SolveDocument12 pagesAntibiotic Solvesami azadNo ratings yet
- Abutment: Pulf L em NoDocument7 pagesAbutment: Pulf L em Nosami azadNo ratings yet
- BDR CaseDocument3 pagesBDR Casesami azadNo ratings yet
- Priya Verma Gupta, Amitha M. Hegde - Pediatric Dentistry For Special Child (2015, Jaypee Brothers Medical Pub) PDFDocument493 pagesPriya Verma Gupta, Amitha M. Hegde - Pediatric Dentistry For Special Child (2015, Jaypee Brothers Medical Pub) PDFsami azadNo ratings yet
- Covid 19 022020Document11 pagesCovid 19 022020Pouronik KarmakerNo ratings yet
- The Milk LetterDocument14 pagesThe Milk LetterLily SimpsonNo ratings yet
- FMCG Mind Map by HCHDocument6 pagesFMCG Mind Map by HCHHEMANTH VENKATA MANI SAI CHINTALANo ratings yet
- Reesearch (Related Literature) Care of Older AdultsDocument105 pagesReesearch (Related Literature) Care of Older AdultsGavebriel MarianoNo ratings yet
- National Immunization ProgramDocument67 pagesNational Immunization ProgrameezahNo ratings yet
- MASTURBATION A Touchy Subject PDFDocument10 pagesMASTURBATION A Touchy Subject PDFMohammed sabeelNo ratings yet
- Increasing crop diversity and food distribution to address malnutrition in IndonesiaDocument7 pagesIncreasing crop diversity and food distribution to address malnutrition in Indonesia221 Rafly Rahmadafa SyabaniNo ratings yet
- Brendan Morano Final EvaluationDocument15 pagesBrendan Morano Final Evaluationapi-546391110No ratings yet
- Mild Cognitive Impairment Continuum 2016Document15 pagesMild Cognitive Impairment Continuum 2016Habib G. Moutran BarrosoNo ratings yet
- Pharmacrystal BoucherDocument14 pagesPharmacrystal BoucherAmit Patel100% (1)
- Huntington's Disease TBLDocument4 pagesHuntington's Disease TBLlalee704No ratings yet
- Saving Lives Averting CostsDocument79 pagesSaving Lives Averting CostsMedCR1987No ratings yet
- Global Health Initiatives Lesson PlanDocument2 pagesGlobal Health Initiatives Lesson PlanJoshua Guiriña82% (11)
- Bio Magnetism - Future of HealthDocument32 pagesBio Magnetism - Future of HealthProf. Madhavan100% (15)
- Guidelines For Prescribing Radiographs. Neill SermanDocument7 pagesGuidelines For Prescribing Radiographs. Neill Sermandddemourita9249No ratings yet
- Primary Eye Care Concepts and ComponentsDocument3 pagesPrimary Eye Care Concepts and ComponentsAreenaNo ratings yet
- ATP Blog - Things To Know About Fulvic AcidDocument17 pagesATP Blog - Things To Know About Fulvic Acidatpfacebook100% (1)
- 24 Spirofy 8 PG Pda - 230913 - 102157Document4 pages24 Spirofy 8 PG Pda - 230913 - 102157Amit KaradNo ratings yet
- Sop PDFDocument2 pagesSop PDFTahsina TabassumNo ratings yet
- Chu2018 OBESITY ImpDocument19 pagesChu2018 OBESITY ImpPoonam joshiNo ratings yet
- Covid 19 TreatmentDocument2 pagesCovid 19 TreatmentGio Tamaño BalisiNo ratings yet
- Vitamin D Deficiency and Anemia Among Pharmacy StudentsDocument7 pagesVitamin D Deficiency and Anemia Among Pharmacy StudentsMediterr J Pharm Pharm SciNo ratings yet
- Vital Scoop BWDocument4 pagesVital Scoop BWLis4cgNo ratings yet
- Sport Safety and Emergency PlanDocument4 pagesSport Safety and Emergency PlanReynan Posada TapiaNo ratings yet
- Imei UrinanalysisDocument3 pagesImei UrinanalysisRohitNo ratings yet
- Assignment DNHEDocument9 pagesAssignment DNHEmohitNo ratings yet
- Policies and Procedures On Outsourced Ancillary ServicesDocument2 pagesPolicies and Procedures On Outsourced Ancillary ServicesEdison MartinezNo ratings yet
- Nutrition Now 8th Edition Brown Solutions Manual 1Document36 pagesNutrition Now 8th Edition Brown Solutions Manual 1codyschultzetrksicgjn100% (24)
- Innovations in NursingDocument14 pagesInnovations in NursingDelphy Varghese100% (1)
- Positioning Child Cerebral Palsy Posture ControlDocument8 pagesPositioning Child Cerebral Palsy Posture ControlAdnan RezaNo ratings yet
- NZ Mini-ACE Administration and Scoring Guide 2020Document6 pagesNZ Mini-ACE Administration and Scoring Guide 2020madalinaNo ratings yet