You might also like
- Excess Deaths Involving CVD in England An Anlysis and ExplainerDocument36 pagesExcess Deaths Involving CVD in England An Anlysis and ExplainerJamie White100% (2)
- 6 B&B CirrhosisDocument30 pages6 B&B CirrhosisSara Joseph100% (1)
- Hemiplegia Rehabilitation TechniquesDocument11 pagesHemiplegia Rehabilitation TechniquesFares EL DeenNo ratings yet
- VAC - Barangay Data Capture FormDocument1 pageVAC - Barangay Data Capture Formboy100% (1)
- Anatomy & Physiology of The Cardiovascular SystemDocument3 pagesAnatomy & Physiology of The Cardiovascular SystemluaNo ratings yet
- Superficial and Deep ReflexesDocument28 pagesSuperficial and Deep ReflexesShilpa SNo ratings yet
- MCQDocument4 pagesMCQEliza SparkNo ratings yet
- Colloids and CrystalooidsDocument42 pagesColloids and Crystalooidsلؤي زعيترNo ratings yet
- NCP #2Document2 pagesNCP #2Faith CalimlimNo ratings yet
- Oxygen Therapy AdministrationDocument15 pagesOxygen Therapy AdministrationMike Faustino Solangon100% (1)
- OSCE Station 1 Diabetic LL ExamDocument5 pagesOSCE Station 1 Diabetic LL ExamJeremy YangNo ratings yet
- Quiz With AnswersDocument8 pagesQuiz With Answersval284yNo ratings yet
- ScienceDocument17 pagesScienceTambong HailyNo ratings yet
- Abdominal Examination Check ListDocument9 pagesAbdominal Examination Check ListIbrahim Ahmed IbrahimNo ratings yet
- 780 Adult Cardio Resp Assess DSTDocument10 pages780 Adult Cardio Resp Assess DSTGursangeet Kaur100% (1)
- NCLEX Practice Questions Quiz #4: Fundamentals of NursingDocument12 pagesNCLEX Practice Questions Quiz #4: Fundamentals of NursingRegine Mae Encinada100% (1)
- Cor Pulmonale Lesson PlanDocument49 pagesCor Pulmonale Lesson PlanRadha Sri50% (2)
- Multiple Sclerosis Nursing Care GuideDocument5 pagesMultiple Sclerosis Nursing Care GuideNoelyn BaluyanNo ratings yet
- Types of Seizure & Status Epilepticus: Prepared By: Ivy Joy A. Benitez, BSN 4-ADocument28 pagesTypes of Seizure & Status Epilepticus: Prepared By: Ivy Joy A. Benitez, BSN 4-AyviyojNo ratings yet
- Assessment of Cardiovascular SystemDocument5 pagesAssessment of Cardiovascular SystemAnamika ChoudharyNo ratings yet
- Head InjuryDocument22 pagesHead InjuryNguyễn Ly100% (1)
- SHOCKDocument35 pagesSHOCKsami azadNo ratings yet
- 1 - Introduction To Gastroenterology (2) SlaytDocument31 pages1 - Introduction To Gastroenterology (2) SlaytZeynep ArasNo ratings yet
- Post Operative HemorrhageDocument16 pagesPost Operative Hemorrhagenishimura89No ratings yet
- GCNM - Lecture 1Document45 pagesGCNM - Lecture 1itsukoNo ratings yet
- Main Applications of ECG DiagnosisDocument19 pagesMain Applications of ECG DiagnosisMaria Rowena O. SalvoNo ratings yet
- EPILEPSY Lecture NoteDocument17 pagesEPILEPSY Lecture Notemohammed awolNo ratings yet
- Compartment Syndrome Diagnosis and TreatmentDocument3 pagesCompartment Syndrome Diagnosis and TreatmentTantyo Adi P100% (2)
- Congestive Heart Failure OverviewDocument12 pagesCongestive Heart Failure OverviewkazelleNo ratings yet
- Medical Mnemonics Memory HacksDocument7 pagesMedical Mnemonics Memory HacksHaseebUl haqNo ratings yet
- Anesthetic Consideration For Patients With Obstructive JaundiceDocument47 pagesAnesthetic Consideration For Patients With Obstructive JaundiceagatakassaNo ratings yet
- Cardiology MCQDocument2 pagesCardiology MCQmohamed mowafeyNo ratings yet
- 02 Bronchial Asthma Circ 2018-2019Document15 pages02 Bronchial Asthma Circ 2018-2019Mooha Alanzy100% (1)
- Nursing Care - TraditionalDocument38 pagesNursing Care - Traditionalchishimba louisNo ratings yet
- Critical Care Environment - Design Stucture and FacilitiesDocument22 pagesCritical Care Environment - Design Stucture and FacilitiesProf. Ramsharan MehtaNo ratings yet
- Nursing Assessment:: Intervention Rationale Independent InterventionsDocument2 pagesNursing Assessment:: Intervention Rationale Independent Interventionsnananana123No ratings yet
- Orientation To Blood Bank 2Document24 pagesOrientation To Blood Bank 2Darshita SharmaNo ratings yet
- Burn Mcqs2Document11 pagesBurn Mcqs2Musa yohanaNo ratings yet
- Bio StatisticsDocument101 pagesBio StatisticshferdjalNo ratings yet
- Ceftriaxone PDFDocument1 pageCeftriaxone PDFveniNo ratings yet
- Muscle Relaxants Classification and Mechanisms of ActionDocument22 pagesMuscle Relaxants Classification and Mechanisms of Actionvinay0717100% (1)
- 21 - Postoperative Complications and Managament IDocument30 pages21 - Postoperative Complications and Managament IAmmarNo ratings yet
- Alata SaminaMCQsDocument132 pagesAlata SaminaMCQsmintahmeshackbenjaminNo ratings yet
- National NORCET Test-8Document108 pagesNational NORCET Test-8SHIVANIINo ratings yet
- Physiology of Hearing: Departemen Fisiologi FK UsuDocument28 pagesPhysiology of Hearing: Departemen Fisiologi FK UsuSonia P SNo ratings yet
- Cardio AssessmentDocument2 pagesCardio AssessmentMabesNo ratings yet
- APPLIANCE 3e (Instruments) - 1Document174 pagesAPPLIANCE 3e (Instruments) - 1Fahad2036100% (2)
- INTUSSUSCEPTIONDocument3 pagesINTUSSUSCEPTIONS GNo ratings yet
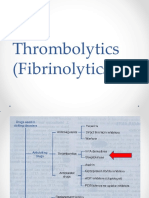
- Thrombolytics (Fibrinolytics)Document14 pagesThrombolytics (Fibrinolytics)J lodhiNo ratings yet
- Pancreatitis: Causes, Symptoms, and TreatmentDocument5 pagesPancreatitis: Causes, Symptoms, and TreatmentSanthu Su100% (2)
- Respiratory Therapy Equipment GuideDocument6 pagesRespiratory Therapy Equipment GuideJack OneNo ratings yet
- Introduction of Pediatric Nursing: Om Nursing Academy Anil Kantiwal Gudha (Whatsapp 9694936335)Document4 pagesIntroduction of Pediatric Nursing: Om Nursing Academy Anil Kantiwal Gudha (Whatsapp 9694936335)Preeti ChouhanNo ratings yet
- PANCREATITISDocument38 pagesPANCREATITISVEDHIKAVIJAYANNo ratings yet
- Preoperative Assessment of Diabetic PatientsDocument2 pagesPreoperative Assessment of Diabetic PatientsShilpa Pradhan100% (1)
- CVP MonitoringDocument24 pagesCVP MonitoringChoji Heiwajima100% (1)
- Post Operative ComplicationsDocument17 pagesPost Operative Complicationsdrhiwaomer100% (8)
- HypothyroidismDocument54 pagesHypothyroidismagakshat23No ratings yet
- Spa PPT - FinalDocument45 pagesSpa PPT - FinalShivam DwivediNo ratings yet
- Asthma Patient ProfileDocument8 pagesAsthma Patient ProfileGlenn Asuncion PagaduanNo ratings yet
- Nursing Care Plan for Client with Major BurnDocument2 pagesNursing Care Plan for Client with Major BurnMaricel R. ManabatNo ratings yet
- Congenital GenitourinaryDocument93 pagesCongenital GenitourinaryEllen AngelNo ratings yet
- Questions 2Document20 pagesQuestions 2Ahwen 'ahwenism'No ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingFrom EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováNo ratings yet
- Pacemaker Therapy-1Document30 pagesPacemaker Therapy-1shejila c hNo ratings yet
- Curriculum Mapping DefinitionDocument3 pagesCurriculum Mapping Definitionshejila c hNo ratings yet
- Cardiomyopathies 1Document19 pagesCardiomyopathies 1shejila c hNo ratings yet
- PCI Procedures ExplainedDocument24 pagesPCI Procedures Explainedshejila c hNo ratings yet
- DraftNursingbill 0Document48 pagesDraftNursingbill 0shejila c hNo ratings yet
- SCNS AguidetoadminscoringanalysesDocument69 pagesSCNS Aguidetoadminscoringanalysesshejila c hNo ratings yet
- NIH Public Access: Innovations That INSPIREDocument4 pagesNIH Public Access: Innovations That INSPIREshejila c hNo ratings yet
- Crozier Et Al INMPP 2012Document10 pagesCrozier Et Al INMPP 2012shejila c hNo ratings yet
- Development of A New Nurse Navigator Program - Journal of Oncology Navigation & SurvivorshipDocument7 pagesDevelopment of A New Nurse Navigator Program - Journal of Oncology Navigation & Survivorshipshejila c hNo ratings yet
- Innovation in Nursing PracticesDocument6 pagesInnovation in Nursing PracticesVijaya RaniNo ratings yet
- GX LSHC Care Model InnovationDocument1 pageGX LSHC Care Model Innovationshejila c hNo ratings yet
- Innovation in Nursing: A Concept Analysis: January 2016Document5 pagesInnovation in Nursing: A Concept Analysis: January 2016shejila c hNo ratings yet
- Febrile Convulsion - SeizuresDocument20 pagesFebrile Convulsion - Seizuressai saiNo ratings yet
- Assessing Jugular Venous Pressure and Cardiovascular SignsDocument15 pagesAssessing Jugular Venous Pressure and Cardiovascular SignscianixNo ratings yet
- 491.prevention of Heart Attacks & Cardiovascular DiseasesDocument80 pages491.prevention of Heart Attacks & Cardiovascular DiseasesAlberto Mora PereaNo ratings yet
- Nursing care plan for post-op cataract surgeryDocument2 pagesNursing care plan for post-op cataract surgeryFranz goNo ratings yet
- Wepik Minimalist Occupational Therapy Services Brochure 20231115022536YWFXDocument2 pagesWepik Minimalist Occupational Therapy Services Brochure 20231115022536YWFXMuhd Afif HilmiNo ratings yet
- Trauma in ChildrenDocument11 pagesTrauma in ChildrenEdwardRazvanNo ratings yet
- Penatalaksanaan Petugas Terpapar COVID-19Document30 pagesPenatalaksanaan Petugas Terpapar COVID-19Taupick ArsyNo ratings yet
- Allium CepaDocument8 pagesAllium CepaAru VermaNo ratings yet
- Color Doppler Flow Imaging of Retrobulbar Ocular Blood Flow Changes in Retinal Artery Occlusions Caused by Cosmetic Facial Filler InjectionsDocument5 pagesColor Doppler Flow Imaging of Retrobulbar Ocular Blood Flow Changes in Retinal Artery Occlusions Caused by Cosmetic Facial Filler InjectionsKerlida SantosNo ratings yet
- Aortic AneurysmDocument60 pagesAortic AneurysmSantosh NaliathNo ratings yet
- Peoria County Booking Sheet 04/02/14Document11 pagesPeoria County Booking Sheet 04/02/14Journal Star police documentsNo ratings yet
- DKA Texas Children 19Document9 pagesDKA Texas Children 19Eduardo RuizNo ratings yet
- Ra 9262Document43 pagesRa 9262Kim ZeNo ratings yet
- GI QuestionsDocument3 pagesGI QuestionsYusif ElmiNo ratings yet
- Lecture9-Nutrition and CancerDocument65 pagesLecture9-Nutrition and Cancermirabel IvanaliNo ratings yet
- Severe Anxiety Case StudyDocument2 pagesSevere Anxiety Case StudyCamille SindayNo ratings yet
- Bài Thi Onl Lư NG T PDFDocument3 pagesBài Thi Onl Lư NG T PDFVõ Nguyễn Kiều TrinhNo ratings yet
- An Assignment: Course Name: Course No.: PHY-5213Document5 pagesAn Assignment: Course Name: Course No.: PHY-5213Tonmoy PaulNo ratings yet
- Introduction in Skeletal System1Document11 pagesIntroduction in Skeletal System1joana cortezNo ratings yet
- ATLS Powerpoint YoDocument29 pagesATLS Powerpoint YobharatNo ratings yet
- Orem Theory FractureDocument4 pagesOrem Theory FractureHadeer HamdyNo ratings yet
- Praseno Hadi - ARDS (Malang 2018)Document25 pagesPraseno Hadi - ARDS (Malang 2018)Rian HutabaratNo ratings yet
- Off Tag Assessment (Surgery)Document19 pagesOff Tag Assessment (Surgery)Ahmad LiewNo ratings yet
- Advances in Cancer Immunotherapy 2019 - Latest TrendsDocument21 pagesAdvances in Cancer Immunotherapy 2019 - Latest TrendsSWAGATIKA CHANDANo ratings yet
- Head and Neck NCPDocument2 pagesHead and Neck NCPAngelo AbiganiaNo ratings yet