You might also like
- Sewing Machines Training ManualDocument20 pagesSewing Machines Training ManualGashaw Fikir AdugnaNo ratings yet
- History of Madre de DiosDocument3 pagesHistory of Madre de DiosMisterJanNo ratings yet
- The Greenock HangingsDocument5 pagesThe Greenock HangingsInverclyde Community Development Trust100% (2)
- List of All ProjectsDocument152 pagesList of All ProjectsMhm ReddyNo ratings yet
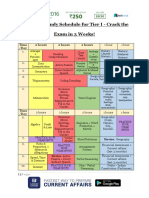
- SSC CHSL Study Schedule For Tier I - Crack The Exam in 3 Weeks!Document3 pagesSSC CHSL Study Schedule For Tier I - Crack The Exam in 3 Weeks!Tushita80% (15)
- Grade-9 (1st)Document42 pagesGrade-9 (1st)Jen Ina Lora-Velasco GacutanNo ratings yet
- Landscape Architecture: Elements of Garden DesignDocument7 pagesLandscape Architecture: Elements of Garden Designtwinkle4545No ratings yet
- User Manual: Shenzhen Biocare Bio-Medical Equipment Co., LTDDocument182 pagesUser Manual: Shenzhen Biocare Bio-Medical Equipment Co., LTDArnaldo AbadNo ratings yet
- Introduction To Industrial EcologyDocument107 pagesIntroduction To Industrial EcologyMohamed AliNo ratings yet
- Handbook of Environmental Data and Ecological Parameters: Environmental Sciences and ApplicationsFrom EverandHandbook of Environmental Data and Ecological Parameters: Environmental Sciences and ApplicationsS. E. JørgensenNo ratings yet
- Chan (2011)Document8 pagesChan (2011)Jorge Andres Molina GonzalezNo ratings yet
- Prediction of Soil Organic Carbon For Ethiopian Hi PDFDocument13 pagesPrediction of Soil Organic Carbon For Ethiopian Hi PDFTiruneh GANo ratings yet
- Recipe 2008Document133 pagesRecipe 2008Marcela RuizNo ratings yet
- Kiểm kê phát thải theo không gian và thời gian đốt tàn dư cây trồng trên cánh đồngDocument12 pagesKiểm kê phát thải theo không gian và thời gian đốt tàn dư cây trồng trên cánh đồngptthuy0723No ratings yet
- Adsorption of CrVI Ions Onto Goethite Activated CaDocument18 pagesAdsorption of CrVI Ions Onto Goethite Activated CaDella KharismaNo ratings yet
- Environmental Pollution: SciencedirectDocument9 pagesEnvironmental Pollution: SciencedirectAnel Viridiana Alfonso BocarandoNo ratings yet
- Schedule of Lecture by Jiro Takemura: "Geoenvironmental Engineering"Document7 pagesSchedule of Lecture by Jiro Takemura: "Geoenvironmental Engineering"Mohammad NamaeeNo ratings yet
- 1 s2.0 S0959652620355141 MainDocument14 pages1 s2.0 S0959652620355141 Mainalfadjrii syahhhNo ratings yet
- Iogas Production by Means of An Anaerobic-Digestion Plant in France LCA of Greenhouse-Gas Emissions and Other Environmental Indicators.Document14 pagesIogas Production by Means of An Anaerobic-Digestion Plant in France LCA of Greenhouse-Gas Emissions and Other Environmental Indicators.Karin yardely Tafur huayanNo ratings yet
- Gbemisola Et AlDocument6 pagesGbemisola Et AlTraian BarbuNo ratings yet
- Yun 2020Document10 pagesYun 2020amira mansourkhodjaNo ratings yet
- Ajol File Journals - 82 - Articles - 71343 - Submission - Proof - 71343 973 154063 1 10 20111027Document6 pagesAjol File Journals - 82 - Articles - 71343 - Submission - Proof - 71343 973 154063 1 10 20111027may.alvesouzaNo ratings yet
- Jurnal Inter Acara 3Document7 pagesJurnal Inter Acara 3Kelvin ZainNo ratings yet
- CarbonFootprintEvaluationandReductionasaClimateChangeMitigationTool CaseStudyofFederalUniversityofAgricultureAbeokutaOgunStateNigeriaDocument7 pagesCarbonFootprintEvaluationandReductionasaClimateChangeMitigationTool CaseStudyofFederalUniversityofAgricultureAbeokutaOgunStateNigeriaJuventie PrimastutiNo ratings yet
- Evaluation and Comparison of MODIS Collection 61 ADocument18 pagesEvaluation and Comparison of MODIS Collection 61 AKobi AhsanNo ratings yet
- City-Level Carbon Emission Abatement in The Subtropics of China: Evaluation and Reallocation For ZhejiangDocument12 pagesCity-Level Carbon Emission Abatement in The Subtropics of China: Evaluation and Reallocation For ZhejiangChenpeng FENGNo ratings yet
- Ekc 5Document11 pagesEkc 5Navjot PannuNo ratings yet
- 1 s2.0 S0921344903001204 MainDocument17 pages1 s2.0 S0921344903001204 MainFitaTriWantikaNo ratings yet
- 1 s2.0 S0045653512012660 MainDocument7 pages1 s2.0 S0045653512012660 MainJennNo ratings yet
- Sustainable Energy Development From Ther PDFDocument9 pagesSustainable Energy Development From Ther PDFSUNNY KANTNo ratings yet
- 710 2733 1 PBDocument9 pages710 2733 1 PBrizkyaa678No ratings yet
- Benvironment Statistics of Nepal 2019 PDFDocument257 pagesBenvironment Statistics of Nepal 2019 PDFसुनिल बाबु खत्रीNo ratings yet
- Food Chemistry 333 (2020) 127495Document9 pagesFood Chemistry 333 (2020) 127495Luminita AndronicNo ratings yet
- Influence of Environmental PollutionDocument5 pagesInfluence of Environmental PollutionPauldennis7No ratings yet
- Uba and Basil Publication 2Document9 pagesUba and Basil Publication 2Bright UbaNo ratings yet
- 1 PBDocument6 pages1 PBbernabasNo ratings yet
- Continuous Adsorption of A Cationic Dye On Surface Modified Rice Husk Statistical Optimization and Dynamic ModelsDocument11 pagesContinuous Adsorption of A Cationic Dye On Surface Modified Rice Husk Statistical Optimization and Dynamic ModelsDison FrancoNo ratings yet
- Ecotoxicology and Environmental Safety: Penggang Pei, Yuebing Sun, Lin Wang, Xuefeng Liang, Yingming XuDocument11 pagesEcotoxicology and Environmental Safety: Penggang Pei, Yuebing Sun, Lin Wang, Xuefeng Liang, Yingming XuUlfa Mudia SariNo ratings yet
- Air Quality Monitoring in Industrial Area of Orchard Street, Batam CityDocument5 pagesAir Quality Monitoring in Industrial Area of Orchard Street, Batam Citytl201kd2No ratings yet
- Estimation and Mapping of Carbon Stocks in Bosomkese Forest ReserveDocument12 pagesEstimation and Mapping of Carbon Stocks in Bosomkese Forest ReserveSEP-PublisherNo ratings yet
- Green Synthesis of Silver Nanoparticles Using An 2017 Saudi Journal of BioloDocument6 pagesGreen Synthesis of Silver Nanoparticles Using An 2017 Saudi Journal of Bioloshiba meike indiraNo ratings yet
- Ogah Et Al 2020Document7 pagesOgah Et Al 2020Egah GodwinNo ratings yet
- CSTEP Source Apportionment Study For Bengaluru 21feb2022Document142 pagesCSTEP Source Apportionment Study For Bengaluru 21feb2022shubham1234262No ratings yet
- Intercomparison of Methods To Estimate Black Carbon EmissionsDocument8 pagesIntercomparison of Methods To Estimate Black Carbon EmissionsJoy RoyNo ratings yet
- Universitas Pertamina, IndonesiaDocument11 pagesUniversitas Pertamina, IndonesiaOctavio Manuel Ibacache VelasquezNo ratings yet
- Computational Pollutant of So2/no2 in The Environment Using Aermod in Semi-Urban Area, Studi Case in Tuban, East JavaDocument6 pagesComputational Pollutant of So2/no2 in The Environment Using Aermod in Semi-Urban Area, Studi Case in Tuban, East JavaIJAR JOURNALNo ratings yet
- Proposal SlidesDocument13 pagesProposal SlidesOluwatobiloba IbrahimNo ratings yet
- Procedia EnvironmentalDocument8 pagesProcedia EnvironmentalYossy RyanantaNo ratings yet
- Khoo 2010Document7 pagesKhoo 2010Annisa WisdayatiNo ratings yet
- Application of Arac Á Fruit Husks (Psidium in The Preparation of Activated Carbon With Fecl For Atrazine Herbicide AdsorptionDocument12 pagesApplication of Arac Á Fruit Husks (Psidium in The Preparation of Activated Carbon With Fecl For Atrazine Herbicide AdsorptionCarolinne FerronatoNo ratings yet
- Reinhard Lovell Thijs Se Nej or 2000Document18 pagesReinhard Lovell Thijs Se Nej or 2000zdenkaNo ratings yet
- MY Letter Guideliness and Application Form For BE & ME Proje 2017-20Document7 pagesMY Letter Guideliness and Application Form For BE & ME Proje 2017-20PRAKASH KUMARNo ratings yet
- Efficiency of Gamma Radiation Technology in DecontDocument6 pagesEfficiency of Gamma Radiation Technology in DecontMoe Abdul'sNo ratings yet
- Atmospheric Environment: Ekbordin Winijkul, Laura Fierce, Tami C. BondDocument14 pagesAtmospheric Environment: Ekbordin Winijkul, Laura Fierce, Tami C. BondNebojsa RedzicNo ratings yet
- Presentation On Review Paper PDFDocument21 pagesPresentation On Review Paper PDFALI ANWARNo ratings yet
- Accumulation of Metabolic Carbon Dioxide (CO2) in A Vehicle CabinDocument7 pagesAccumulation of Metabolic Carbon Dioxide (CO2) in A Vehicle CabinlowwallNo ratings yet
- Carbon SequestrationDocument10 pagesCarbon SequestrationYob YnnosNo ratings yet
- Abdallah 2020Document10 pagesAbdallah 2020Piotr KucharskiNo ratings yet
- AGRONOMY-27-Thorburn Emisiones NDocument9 pagesAGRONOMY-27-Thorburn Emisiones NMari Paz Conejo ArayaNo ratings yet
- Prediction of Regional Agro-Industrial Wastes Characteristics by Thermogravimetric Analysis To Obtain Bioenergy Using Thermal ProcessDocument14 pagesPrediction of Regional Agro-Industrial Wastes Characteristics by Thermogravimetric Analysis To Obtain Bioenergy Using Thermal ProcessirNo ratings yet
- Chemosphere: Ville Turunen, Jaana Sorvari, Anna MikolaDocument9 pagesChemosphere: Ville Turunen, Jaana Sorvari, Anna MikolaCarlos AlvarezNo ratings yet
- Carbon Footprint AnalysisDocument18 pagesCarbon Footprint AnalysisAndres AndradeNo ratings yet
- Atmospheric EnvironmentDocument8 pagesAtmospheric EnvironmentSarup Das ce20d036No ratings yet
- qt3dv1d6xv NosplashDocument67 pagesqt3dv1d6xv NosplashFahad kamranNo ratings yet
- 2 Analysis of Cabon FootprintDocument22 pages2 Analysis of Cabon FootprintdivyaNo ratings yet
- A Computational Model For Soil Fertility Prediction in Ubiquitous AgricultureDocument9 pagesA Computational Model For Soil Fertility Prediction in Ubiquitous AgricultureflaviorochaavilaNo ratings yet
- Assessment of Windrow Composting Plant's Performance at Keru, Jodhpur, IndiaDocument5 pagesAssessment of Windrow Composting Plant's Performance at Keru, Jodhpur, IndiaKalyan ReddyNo ratings yet
- 1 s2.0 S0959652620355104 MainDocument13 pages1 s2.0 S0959652620355104 MainkendlpNo ratings yet
- 3.1 Nature of Enzymes: UNIT-3 3. Enzymes 1. Catalytic PropertyDocument5 pages3.1 Nature of Enzymes: UNIT-3 3. Enzymes 1. Catalytic PropertyGashaw Fikir AdugnaNo ratings yet
- III-3-3-2 PDCA Cycle Is Golden Cycle For KAIZEN: Past Performances or Future Forecasting of WorkDocument33 pagesIII-3-3-2 PDCA Cycle Is Golden Cycle For KAIZEN: Past Performances or Future Forecasting of WorkGashaw Fikir AdugnaNo ratings yet
- Grade 12 ch1 & ch2 BioDocument12 pagesGrade 12 ch1 & ch2 BioGashaw Fikir AdugnaNo ratings yet
- ABDI Last Resarch111resarche11-1Document61 pagesABDI Last Resarch111resarche11-1Gashaw Fikir AdugnaNo ratings yet
- Secondary School Biology Short Notes and Exercises For Grade 9Document19 pagesSecondary School Biology Short Notes and Exercises For Grade 9Gashaw Fikir AdugnaNo ratings yet
- Secondary School Biology Short Notes and Exercises For Grade 10Document22 pagesSecondary School Biology Short Notes and Exercises For Grade 10Gashaw Fikir AdugnaNo ratings yet
- Fgc-Chapter OneDocument30 pagesFgc-Chapter OneGashaw Fikir AdugnaNo ratings yet
- Chapter One - FTVETIDocument84 pagesChapter One - FTVETIGashaw Fikir AdugnaNo ratings yet
- Factor of Fashion PDFDocument11 pagesFactor of Fashion PDFGashaw Fikir AdugnaNo ratings yet
- Factor of Fashion PDFDocument11 pagesFactor of Fashion PDFGashaw Fikir AdugnaNo ratings yet
- Internal Guide-BE Project Groups 2015-16Document28 pagesInternal Guide-BE Project Groups 2015-16Aravind IyerNo ratings yet
- Baughman Don Marianne 1977 NigeriaDocument11 pagesBaughman Don Marianne 1977 Nigeriathe missions networkNo ratings yet
- Moskvin Eng FibromialgiaDocument218 pagesMoskvin Eng FibromialgiaWebster LimNo ratings yet
- From St. Francis To Dante-Translations From The Chronicle of The Franciscan Salimbene, 1221-1288Document489 pagesFrom St. Francis To Dante-Translations From The Chronicle of The Franciscan Salimbene, 1221-1288Jake SalNo ratings yet
- Bernardo Carpio - Mark Bryan NatontonDocument18 pagesBernardo Carpio - Mark Bryan NatontonMark Bryan NatontonNo ratings yet
- Present Perfect TestDocument6 pagesPresent Perfect TestMárta FábiánNo ratings yet
- Lguvisitation-Municipality of CaintaDocument23 pagesLguvisitation-Municipality of CaintaDaniel BulanNo ratings yet
- Evija - Lotus Cars Official WebsiteDocument5 pagesEvija - Lotus Cars Official WebsiteluyuanNo ratings yet
- 5990200Document551 pages5990200Basit Ahmad bhat0% (1)
- PMLS 2 Unit 9Document3 pagesPMLS 2 Unit 9Elyon Jirehel AlvarezNo ratings yet
- Wimod Ic iC880A: DatasheetDocument26 pagesWimod Ic iC880A: DatasheetJulian CamiloNo ratings yet
- SSLD Stairways LowresDocument44 pagesSSLD Stairways LowresboyNo ratings yet
- Catalogue2019 PDFDocument12 pagesCatalogue2019 PDFlakavath arthiNo ratings yet
- AOP Lecture Sheet 01Document7 pagesAOP Lecture Sheet 01Nakib Ibna BasharNo ratings yet
- Holy Is The Lord-GDocument1 pageHoly Is The Lord-Gmolina.t4613No ratings yet
- CW-80 ManualDocument12 pagesCW-80 ManualBrian YostNo ratings yet
- Technical Support Questions and Answers: How Do I Access Commseciress?Document3 pagesTechnical Support Questions and Answers: How Do I Access Commseciress?goviperumal_33237245No ratings yet
- 131101-2 Gtu 3rd Sem PaperDocument4 pages131101-2 Gtu 3rd Sem PaperShailesh SankdasariyaNo ratings yet
- Book Review - 1: Reviewer: Devajyoti BiswasDocument3 pagesBook Review - 1: Reviewer: Devajyoti BiswassaemoonNo ratings yet
- Attention and Effort. (1973)Document253 pagesAttention and Effort. (1973)Robert C. CasasNo ratings yet
- Separation of Powers - WikipediaDocument15 pagesSeparation of Powers - WikipediaSacredly YoursNo ratings yet
- 2006 Amc8Document12 pages2006 Amc8Yuhang HeNo ratings yet
- Forest Field Trip ReportDocument8 pagesForest Field Trip Reportapi-296213542100% (2)