You might also like
- Cubital Tunnel Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCubital Tunnel Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- DjfhgoiefkDocument32 pagesDjfhgoiefkhoseajeremiaNo ratings yet
- Cervical Root Syndrome Sc4Document50 pagesCervical Root Syndrome Sc4Anang FajarNo ratings yet
- Case ICM I Week 4 JumatDocument3 pagesCase ICM I Week 4 JumatnaynaNo ratings yet
- Cervical RadiculopathyDocument110 pagesCervical RadiculopathyShabana AfzalNo ratings yet
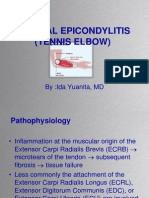
- Lateral Epicondylitis (Tennis Elbow) : By:Ida Yuanita, MDDocument37 pagesLateral Epicondylitis (Tennis Elbow) : By:Ida Yuanita, MDAnang FajarNo ratings yet
- Shoulder pain diagnosis in diabetes patientTITLEDocument67 pagesShoulder pain diagnosis in diabetes patientTITLEmark tNo ratings yet
- CASE STUDY AND QUESTIONS: To Be Completed by The 9th August Week 4: Case 4: AmberDocument7 pagesCASE STUDY AND QUESTIONS: To Be Completed by The 9th August Week 4: Case 4: Amberapi-479499469No ratings yet
- Exercise 1: CHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 7Document5 pagesExercise 1: CHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 7api-453771787No ratings yet
- Soap Note Sub-Acute TkaDocument6 pagesSoap Note Sub-Acute Tkaapi-3719716000% (1)
- Schuster AthleticPelvisDocument26 pagesSchuster AthleticPelvisTheScribbl3rNo ratings yet
- Week 4 Case 4 Chir13009Document6 pagesWeek 4 Case 4 Chir13009api-502504563No ratings yet
- Musculoskeletal Cases For Finals: DR Alastair Brown ST1 Neurosurgery CXHDocument38 pagesMusculoskeletal Cases For Finals: DR Alastair Brown ST1 Neurosurgery CXHAravind RaviNo ratings yet
- Shoulder, Knee & Elbow Injuries GuideDocument13 pagesShoulder, Knee & Elbow Injuries Guidefaria ashrafNo ratings yet
- Systemics Final OP Special Tests and WrittenDocument12 pagesSystemics Final OP Special Tests and WrittenJoanna HuangNo ratings yet
- Week 4 Case 4 Chir13009Document11 pagesWeek 4 Case 4 Chir13009api-468597987No ratings yet
- Week 4 Case 4 Chiro 2020Document11 pagesWeek 4 Case 4 Chiro 2020api-479783350No ratings yet
- Examination of ElbowDocument18 pagesExamination of Elbowharmohit singhNo ratings yet
- Camptodactyly: Amalia Irsha Adhari (1506668510) Eldesta Nisa Nabila (1406642233)Document38 pagesCamptodactyly: Amalia Irsha Adhari (1506668510) Eldesta Nisa Nabila (1406642233)Amalia IrshaNo ratings yet
- Week 4 Case 4 Chir13009Document9 pagesWeek 4 Case 4 Chir13009api-479754549No ratings yet
- Week 4 Case 4 PCP 2Document6 pagesWeek 4 Case 4 PCP 2api-512652362No ratings yet
- CRS Cervical RadiculopathyDocument57 pagesCRS Cervical RadiculopathyBackup WA ORINo ratings yet
- Diagnosis and Management of Ulnar Nerve PalsyDocument20 pagesDiagnosis and Management of Ulnar Nerve PalsyamaliafarahNo ratings yet
- Week 4 Case 4 Chir13009Document9 pagesWeek 4 Case 4 Chir13009api-479720222No ratings yet
- Supracondylar Fractures: Bui Thi Huong Group 6-Y3B Saint Paul HospitalDocument24 pagesSupracondylar Fractures: Bui Thi Huong Group 6-Y3B Saint Paul HospitalHườngNo ratings yet
- Nerve Injury of Upper LimbDocument41 pagesNerve Injury of Upper LimbbashirjnmcNo ratings yet
- Lateral Epicondylitis - Tennis Ellbow HandoutDocument5 pagesLateral Epicondylitis - Tennis Ellbow Handoutgermany23No ratings yet
- Carpal Tunnel Syndrome: by A. A. Sagung Mas CahyandariDocument37 pagesCarpal Tunnel Syndrome: by A. A. Sagung Mas CahyandariAnang FajarNo ratings yet
- Trigger Finger TreatmentDocument33 pagesTrigger Finger TreatmentAnang FajarNo ratings yet
- Lateral Epicondylitis: ST NDDocument2 pagesLateral Epicondylitis: ST NDMuhammad Ucuk100% (1)
- Exercise 1: CHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 5Document8 pagesExercise 1: CHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 5api-455408952No ratings yet
- 242 FullDocument7 pages242 FullParaschiva PîțuNo ratings yet
- Carpal Tunnel SyndromeDocument5 pagesCarpal Tunnel SyndromeCatherine Camille AvelinoNo ratings yet
- Cubital Tunnel Syndrome: Hand & Plastics Physiotherapy DepartmentDocument8 pagesCubital Tunnel Syndrome: Hand & Plastics Physiotherapy DepartmentTorrent IgNo ratings yet
- Cubital Tunnel Syndrome: Hand & Plastics Physiotherapy DepartmentDocument8 pagesCubital Tunnel Syndrome: Hand & Plastics Physiotherapy DepartmentAnonymous VquL3ge6gNo ratings yet
- Golfers Elbow Trigger Point Therapy TreatmentDocument35 pagesGolfers Elbow Trigger Point Therapy TreatmentYes ZamNo ratings yet
- Lab#1 Elbow/Forearm: Examination: PT761.02 M. Briggs PT, DPT, SCS, Atc 4Document8 pagesLab#1 Elbow/Forearm: Examination: PT761.02 M. Briggs PT, DPT, SCS, Atc 4msbriggsNo ratings yet
- Splinting For Peripheral Nerve Injuries-PPT (2023)Document49 pagesSplinting For Peripheral Nerve Injuries-PPT (2023)KarisiNo ratings yet
- Mock 5Document8 pagesMock 5api-364421826No ratings yet
- Case Protocol - SLEDocument9 pagesCase Protocol - SLEGoogle_ajaNo ratings yet
- Cervical SpineDocument177 pagesCervical SpineJayaRakMinimarketNo ratings yet
- Kuda 2Document7 pagesKuda 2HasryaniHaluddinNo ratings yet
- Neck Femur FixDocument20 pagesNeck Femur FixRichard WinardiNo ratings yet
- Week 4 Case 4 Chir13009 Tutors NotesDocument10 pagesWeek 4 Case 4 Chir13009 Tutors Notesapi-502171898No ratings yet
- De Quervain's Tenosynovitis: By: Dr. HermilawatyDocument35 pagesDe Quervain's Tenosynovitis: By: Dr. HermilawatyAnang FajarNo ratings yet
- Anatomy RevisionDocument172 pagesAnatomy RevisionHannah KarlNo ratings yet
- Exercise 1: CHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 7Document4 pagesExercise 1: CHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 7api-479717740No ratings yet
- Exercise 1: CHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 7Document5 pagesExercise 1: CHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 7api-477982644No ratings yet
- Krzywosinski PBLsDocument24 pagesKrzywosinski PBLsleahbayNo ratings yet
- Climbing Injuries Prevention GuideDocument18 pagesClimbing Injuries Prevention GuideDaniel SloskyNo ratings yet
- Long Case OrthopaedicDocument24 pagesLong Case OrthopaedicMorshed Mahbub Abir83% (6)
- All of Surgery IDocument75 pagesAll of Surgery IAli MjadleNo ratings yet
- EBOT. Columna DegenerativaDocument43 pagesEBOT. Columna DegenerativaAna GarridoNo ratings yet
- Examine Cervical Spine Range MotionDocument16 pagesExamine Cervical Spine Range MotionlecturioNo ratings yet
- Supraspinatous Muscle Shoulder PainDocument5 pagesSupraspinatous Muscle Shoulder Painunbelievable686No ratings yet
- David Butler Neural Tissue Mobilisation-1Document11 pagesDavid Butler Neural Tissue Mobilisation-1Himani BhondgeNo ratings yet
- Radial NerveDocument47 pagesRadial NerveFadilla PermataNo ratings yet
- Week 9 Case Study 9 Chir13009Document7 pagesWeek 9 Case Study 9 Chir13009api-479754549No ratings yet
- WK 10-Ques-Ans GH 30 Sep 19Document3 pagesWK 10-Ques-Ans GH 30 Sep 19api-453771787No ratings yet