You might also like
- Taproots Underlying Principles of Milton Erickson's Therapy and Hypnosis - William Hudson O'HanlonDocument100 pagesTaproots Underlying Principles of Milton Erickson's Therapy and Hypnosis - William Hudson O'HanlonPuruf Puf80% (5)
- Hirarc & Aspect ImpactDocument21 pagesHirarc & Aspect ImpactHazru NazriNo ratings yet
- Wasting of Small Muscles of HandDocument38 pagesWasting of Small Muscles of HandSumit Khare75% (4)
- Health PPT - Ways To Build and Keep SchoolDocument17 pagesHealth PPT - Ways To Build and Keep Schoolraymund quinnsNo ratings yet
- Cubital Tunnel Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCubital Tunnel Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Step 3 Form 3 CorrectedDocument41 pagesStep 3 Form 3 CorrectedSBG BPT100% (2)
- Carpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandCarpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- ContractureDocument45 pagesContracturePramitha Yustia100% (1)
- Carpal Tunnel SyndromeDocument38 pagesCarpal Tunnel Syndromereza prayogaNo ratings yet
- Case Study - Seizure2Document12 pagesCase Study - Seizure2Jenny-Ann Baliday100% (1)
- School Action Plan On Adopt-A-School ProgramDocument4 pagesSchool Action Plan On Adopt-A-School ProgramTitser Rock Son89% (9)
- Carpal Tunnel Syndrome FinalDocument4 pagesCarpal Tunnel Syndrome Finalcatherine_suganob6496100% (2)
- MODULE 5: Neurological Infection. Autoimmune and NeuropathiesDocument6 pagesMODULE 5: Neurological Infection. Autoimmune and NeuropathiesClemente AbinesNo ratings yet
- Carpal Tunnel SyndromeDocument22 pagesCarpal Tunnel SyndromeNUR ZAMZAM AZIZAHNo ratings yet
- Carpal Tunnel Syndrome PDFDocument33 pagesCarpal Tunnel Syndrome PDFGethe PutraNo ratings yet
- What Is Carpal Tunnel SyndromeDocument3 pagesWhat Is Carpal Tunnel SyndromerutipuspitaNo ratings yet
- Carpal Tunnel Syndrome: By: Dr. Masoud Shayesteh AzarDocument34 pagesCarpal Tunnel Syndrome: By: Dr. Masoud Shayesteh AzarTri Ramasari Syanggra DewiNo ratings yet
- Aurelio Lyca Mae M. BSN III-D: Carpal Tunnel Syndrome Profressive Case AnalysisDocument9 pagesAurelio Lyca Mae M. BSN III-D: Carpal Tunnel Syndrome Profressive Case Analysis3D - AURELIO, Lyca Mae M.No ratings yet
- Assignment 5 - Fernandez, Dexter IvanDocument1 pageAssignment 5 - Fernandez, Dexter IvanIvan FernandezNo ratings yet
- Carpal Tunnel SyndromeDocument22 pagesCarpal Tunnel SyndromePinimNo ratings yet
- Carpal Tunnel Syndrome Fact SheetDocument6 pagesCarpal Tunnel Syndrome Fact SheetTissa RanatungeNo ratings yet
- Carpal Tunnel SyndromeDocument5 pagesCarpal Tunnel SyndromeBenjo ObsequioNo ratings yet
- Carpal Tunnel Syndrome 3 InforDocument7 pagesCarpal Tunnel Syndrome 3 InforAnonymous uTEAEbugNo ratings yet
- PBL 15Document27 pagesPBL 15AndiMuhYasserNo ratings yet
- Carpal Tunnel SyndormeDocument6 pagesCarpal Tunnel SyndormeMAE THERESE MONICITNo ratings yet
- Carpal Tunnel SyndromeDocument9 pagesCarpal Tunnel SyndromeMaha RajaNo ratings yet
- Case HandDocument2 pagesCase HandUloko ChristopherNo ratings yet
- Case StudyDocument15 pagesCase StudyWincy Faith SalazarNo ratings yet
- Wang 2018Document10 pagesWang 2018ilham Maulana ArifNo ratings yet
- Carpal Tunnel SyndromeDocument17 pagesCarpal Tunnel SyndromeAstrid IndriatiNo ratings yet
- Carpal Tunnel SyndromeDocument15 pagesCarpal Tunnel SyndromeGargi MP100% (1)
- Carpal Tunnel Syndrom Wesam Aljabali - 1Document38 pagesCarpal Tunnel Syndrom Wesam Aljabali - 1مركز ريلاكس للعلاج الطبيعيNo ratings yet
- Complex Regional Pain SyndromeDocument3 pagesComplex Regional Pain SyndromeRini TiaraNo ratings yet
- Diagnosing and Managing Carpal Tunnel Syndrome in Primary CareDocument2 pagesDiagnosing and Managing Carpal Tunnel Syndrome in Primary CareVania Elvira SingkaliNo ratings yet
- Chiropractic Management (Tinnitus and Meniere's Resolved)Document6 pagesChiropractic Management (Tinnitus and Meniere's Resolved)M VanvNo ratings yet
- Carpal Tunnel Syndrome: Clinical ReviewDocument4 pagesCarpal Tunnel Syndrome: Clinical ReviewGoblin HunterNo ratings yet
- Management of Carpal Tunnel SyndromeDocument11 pagesManagement of Carpal Tunnel Syndromevalerie violaNo ratings yet
- Hand & WristDocument56 pagesHand & WristAbdallah Samir Mostafa٢٠١٩٠٢١٥٩No ratings yet
- Patofisiologi CTS 1Document4 pagesPatofisiologi CTS 1Michael DeniNo ratings yet
- Journal Reading CTSDocument27 pagesJournal Reading CTSwillie hardysonNo ratings yet
- Radial Tunnel SyndromeDocument9 pagesRadial Tunnel SyndromeDavid PalashNo ratings yet
- Carpal Tunnel SyndromeDocument5 pagesCarpal Tunnel SyndromeCatherine Camille AvelinoNo ratings yet
- CASE ASSESSMENT AuDocument12 pagesCASE ASSESSMENT AuChesca UrietaNo ratings yet
- Tetanus Disease by SlidesgoDocument31 pagesTetanus Disease by Slidesgoputri diva prinandaNo ratings yet
- Thesis Reza Salman Roghani PDFDocument76 pagesThesis Reza Salman Roghani PDFscoopyNo ratings yet
- Physical Modalities For The Conservative Treatment of Wrist and Hand'sDocument28 pagesPhysical Modalities For The Conservative Treatment of Wrist and Hand'sfilipecorsairNo ratings yet
- Carpal Tunnel SyndromeDocument1 pageCarpal Tunnel SyndromeIndirackshi SundararajanNo ratings yet
- Arciaga, FG - SGDMicroAnaerobesDocument7 pagesArciaga, FG - SGDMicroAnaerobesFG ArciagaNo ratings yet
- AG 8th TermDocument50 pagesAG 8th TermNeelesh PatilNo ratings yet
- Evaluation of The PatientDocument13 pagesEvaluation of The PatientHannah LeiNo ratings yet
- Carpal Tunnel SyndromeDocument8 pagesCarpal Tunnel SyndromesavindcNo ratings yet
- Lateral Epicondylitis.Document11 pagesLateral Epicondylitis.rabia khalidNo ratings yet
- Perempuan Berusia 65 Tahun Dengan Carpal Tunnel Syndrome: Fakultas Kedokteran, Universitas LampungDocument6 pagesPerempuan Berusia 65 Tahun Dengan Carpal Tunnel Syndrome: Fakultas Kedokteran, Universitas LampungelsyamelindaNo ratings yet
- Carpal Tunnel SyndromeDocument15 pagesCarpal Tunnel SyndromeMalueth AnguiNo ratings yet
- Differentiating UE MononeuropathiesDocument27 pagesDifferentiating UE MononeuropathiesAlpacaNo ratings yet
- Carpal Tunnel Syndrome: BMJ (Online) September 2007Document5 pagesCarpal Tunnel Syndrome: BMJ (Online) September 2007Dewi SartikaNo ratings yet
- Carpal Tunnel Syndrome: An Update For The Primary Care PhysicianDocument5 pagesCarpal Tunnel Syndrome: An Update For The Primary Care PhysicianNovia KurniantiNo ratings yet
- Carpal Tunnel SyndromeDocument2 pagesCarpal Tunnel SyndromeHejar A.No ratings yet
- PBL NeuroDocument45 pagesPBL NeuroInsan_aqidNo ratings yet
- Hand Dequervains Release Standard of Care PT BWHDocument12 pagesHand Dequervains Release Standard of Care PT BWHSteven HamiltonNo ratings yet
- By: Nadia H. Djibran 12.16.777.14.134 Pembimbing: Dr. Muh. Ardi Munir, Sp. OTDocument21 pagesBy: Nadia H. Djibran 12.16.777.14.134 Pembimbing: Dr. Muh. Ardi Munir, Sp. OTRiska PermatasariNo ratings yet
- PT Management in Median Nerve InjuryDocument23 pagesPT Management in Median Nerve InjuryAmelia Putri AriyaniNo ratings yet
- Túnel CarpianoDocument9 pagesTúnel CarpianoPaula Noelia BenítezNo ratings yet
- EXP Carpal TunnelDocument7 pagesEXP Carpal TunnelRomelyn OrdillasNo ratings yet
- Ten Principles of Effective Safety Education RevisitedDocument5 pagesTen Principles of Effective Safety Education RevisitedLiamNo ratings yet
- Newmicrosoftofficepowerpointpresentation 160410175058 PDFDocument37 pagesNewmicrosoftofficepowerpointpresentation 160410175058 PDFDevrathNo ratings yet
- Ms SEEMABALAYAN 9 24 2022 7 04 10 PMDocument9 pagesMs SEEMABALAYAN 9 24 2022 7 04 10 PMMohammad Ali NPNo ratings yet
- NCM 105 Nutrition and Diet Therapy Legal MandatesDocument47 pagesNCM 105 Nutrition and Diet Therapy Legal MandatesLea Angel Dominique MacamNo ratings yet
- Basic Nutrition Concepts & Nutrition Indicators: Training Manual For Project Management Unit MembersDocument45 pagesBasic Nutrition Concepts & Nutrition Indicators: Training Manual For Project Management Unit MembersireneNo ratings yet
- Z-TRACK-METHOD ChecklistDocument5 pagesZ-TRACK-METHOD ChecklistDaniela Villanueva RosalNo ratings yet
- Report On Adaptive ClothingDocument8 pagesReport On Adaptive ClothingDivaNo ratings yet
- Final HIV Written ReportDocument19 pagesFinal HIV Written ReportJohara MacasindelNo ratings yet
- Tourist Attractions in TaiwanDocument2 pagesTourist Attractions in TaiwanKASHMEER SHANE CAYATNo ratings yet
- Art 11 - Voluntary Muscle Relaxation Can Mitigate Fatigue.94639Document5 pagesArt 11 - Voluntary Muscle Relaxation Can Mitigate Fatigue.94639Ulyses RamirezNo ratings yet
- Transference Neurosis & Transference Psychosis, de Margaret LittleDocument343 pagesTransference Neurosis & Transference Psychosis, de Margaret Littlececilia.stanisciaNo ratings yet
- New Roles Pharmacists: Value-Based Pay Creates OpportunitiesDocument33 pagesNew Roles Pharmacists: Value-Based Pay Creates OpportunitiesAnonymous EAPbx6No ratings yet
- Medical School Pediatric Department Chairs, Inc.: Notes From The Association ofDocument4 pagesMedical School Pediatric Department Chairs, Inc.: Notes From The Association ofChristian NaranjoNo ratings yet
- Pearson's Correlation Coefficient: BMJ (Online) July 2012Document3 pagesPearson's Correlation Coefficient: BMJ (Online) July 2012Randy Rafael Asencio AlvaradoNo ratings yet
- Text Information and MediaDocument41 pagesText Information and MediaRegine GuavezNo ratings yet
- PATHFit2 Presentation - KTS (1) - 1 PDFDocument23 pagesPATHFit2 Presentation - KTS (1) - 1 PDFArenNo ratings yet
- Guideline Perkeni 2019Document29 pagesGuideline Perkeni 2019Tiens MonisaNo ratings yet
- Https Doc 14 A0 Apps Viewer - GoogleusercontentDocument3 pagesHttps Doc 14 A0 Apps Viewer - GoogleusercontentPriyanka SharmaNo ratings yet
- Task Performance EuthenicsDocument3 pagesTask Performance EuthenicsKimberly MarquezNo ratings yet
- Reproductive System of SwineDocument11 pagesReproductive System of SwineJaskhem LazoNo ratings yet
- Growth Performance of Broilers Fed Different Levels of PrebioticsDocument7 pagesGrowth Performance of Broilers Fed Different Levels of PrebioticsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- I PAaDocument8 pagesI PAaabriaNo ratings yet
- TRF Mapeh 8Document8 pagesTRF Mapeh 8Dhen Velez LargoNo ratings yet
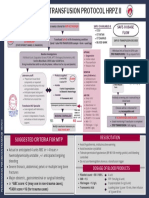
- Final Version MTP Poster 2022 2Document1 pageFinal Version MTP Poster 2022 2Hema Malini ArmugamNo ratings yet
- Benefits of Fucidin CreamDocument2 pagesBenefits of Fucidin CreamErnesto Diaz HernandezNo ratings yet