You might also like
- Care Plan On Acute Transient Psychiatric Disorder 2Document4 pagesCare Plan On Acute Transient Psychiatric Disorder 2Divya ThomasNo ratings yet
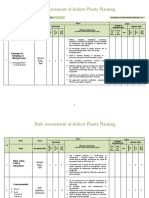
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet
- Schiz NCPDocument5 pagesSchiz NCPCharisse LuteroNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: Short Term Goal: Short Term GoalDocument4 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: Short Term Goal: Short Term Goalmark OrpillaNo ratings yet
- Anupama Ra NotesDocument23 pagesAnupama Ra NotesShahzeel Iftikhar100% (1)
- AdvancedSkillsforComm - BookIDocument96 pagesAdvancedSkillsforComm - BookIfrankito94No ratings yet
- Psychiatric Nursing Care Plan For Schizoaffective DisorderDocument2 pagesPsychiatric Nursing Care Plan For Schizoaffective DisorderChelsea Williams100% (1)
- Factories ActDocument64 pagesFactories ActKrishna Kaushik100% (1)
- (Ebook) SuperBrain Yoga by Master Choa Kok Sui PDFDocument81 pages(Ebook) SuperBrain Yoga by Master Choa Kok Sui PDFBoonyarit Huang100% (5)
- NCP GCS Powerlessness - LIADocument3 pagesNCP GCS Powerlessness - LIADickson,Emilia Jade100% (1)
- Anxiety NCPDocument2 pagesAnxiety NCPAnaleah MalayaoNo ratings yet
- Nursing Care Plan For Situational Low SelfDocument5 pagesNursing Care Plan For Situational Low SelfChar Perea100% (1)
- BD Product ListDocument48 pagesBD Product Listanish_10677953100% (1)
- Jean Pearl R. Caoili Bsn3 NCB Diagnosis: Paranoid Schizophrenia Psychiatric Nursing Care Plan Assessment Explanation of The Problem Goals/ Objectives Interventions Rationale EvaluationDocument9 pagesJean Pearl R. Caoili Bsn3 NCB Diagnosis: Paranoid Schizophrenia Psychiatric Nursing Care Plan Assessment Explanation of The Problem Goals/ Objectives Interventions Rationale Evaluationpj casteNo ratings yet
- List of CosmeticsDocument9 pagesList of Cosmeticsasit_m0% (1)
- Nursing Care Plan For Client With AnxietyDocument2 pagesNursing Care Plan For Client With AnxietyThe Right WayNo ratings yet
- The Subconscious Renaissance: Unleashing, Reprogramming, and Mastering Your Mind for Success and Well-BeingFrom EverandThe Subconscious Renaissance: Unleashing, Reprogramming, and Mastering Your Mind for Success and Well-BeingNo ratings yet
- Paranoid Schizophrenia NCPDocument8 pagesParanoid Schizophrenia NCPCherubim Lei DC Flores67% (3)
- Submitted By: Charisa S. Simbajon BSN IvDocument8 pagesSubmitted By: Charisa S. Simbajon BSN IvCharisa Simbajon100% (1)
- NCP For CSDocument2 pagesNCP For CSIris Coronel AdamosNo ratings yet
- Altered Sensory and Disturbed Thought ProcessDocument4 pagesAltered Sensory and Disturbed Thought ProcessRosecinie Torrente100% (2)
- Disturbed Thought Process NCP Gallano May 22 2018Document3 pagesDisturbed Thought Process NCP Gallano May 22 2018Charles Mallari ValdezNo ratings yet
- Brochure Philippine Laws On Environmental PollutionDocument8 pagesBrochure Philippine Laws On Environmental PollutionElvin JuniorNo ratings yet
- NCP001 IsolationDocument2 pagesNCP001 IsolationJoyh LasutaNo ratings yet
- NCP Alzheimers DiseaseDocument2 pagesNCP Alzheimers DiseaseShawn TejanoNo ratings yet
- NCP-Alzheimer's Disease (Caguimbay)Document9 pagesNCP-Alzheimer's Disease (Caguimbay)Christine Claire CaguimbayNo ratings yet
- Cues Nursing Diagnosis Outcome Nursingintervention Rationale Evaluation Discharge PlanningDocument5 pagesCues Nursing Diagnosis Outcome Nursingintervention Rationale Evaluation Discharge PlanningBSN 3B-Bulatao,Goergie Ann L. CPUSNNo ratings yet
- Schizophrenia NCP and DrugstudyDocument11 pagesSchizophrenia NCP and DrugstudyElle Monge100% (2)
- Intrebari Interviu Asistent MedicalDocument3 pagesIntrebari Interviu Asistent MedicalanaNo ratings yet
- Nursing Care Plan Cues Nursing Diagnosis Objectives Interventions Rationale EvaluationDocument2 pagesNursing Care Plan Cues Nursing Diagnosis Objectives Interventions Rationale EvaluationLi Luren Raphaelle TanNo ratings yet
- Nursing Diagnosis: Disturbed Thought ProcessDocument2 pagesNursing Diagnosis: Disturbed Thought ProcessMelvin PadullaNo ratings yet
- NCP1Document2 pagesNCP1Darlene LaudeNo ratings yet
- NCP 2Document1 pageNCP 2Darlene LaudeNo ratings yet
- Potential Nursing Care Plan SchizopremiaDocument1 pagePotential Nursing Care Plan SchizopremiaopxNo ratings yet
- Urdaneta City University College of NursingDocument2 pagesUrdaneta City University College of NursingSandra ManzanoNo ratings yet
- Assessment Diagnosis Planning Interventions Rationale Evaluation Subjectives: Short-Term GoalDocument5 pagesAssessment Diagnosis Planning Interventions Rationale Evaluation Subjectives: Short-Term Goalmark OrpillaNo ratings yet
- Complicated Grief NCPDocument2 pagesComplicated Grief NCPChristine LebicoNo ratings yet
- Schizophrenia NCPDocument6 pagesSchizophrenia NCPMark EvangelioNo ratings yet
- ANGEL-NCP - CaseloadDocument7 pagesANGEL-NCP - CaseloadNik Rose ElNo ratings yet
- NCP SchizDocument12 pagesNCP SchizKristine Reyes - MerleNo ratings yet
- Care Plan UndifferentiatedDocument11 pagesCare Plan Undifferentiatedilakkiya ilakkiyaNo ratings yet
- Nursing Care Plan IIDocument4 pagesNursing Care Plan IIHarlene Joyce ReyNo ratings yet
- NCP Michael FloresDocument1 pageNCP Michael FloresKyle Audrie ArcalasNo ratings yet
- 7 Modified Communication TechniquesDocument25 pages7 Modified Communication TechniquesmarlonNo ratings yet
- Hallucinations NCP PDFDocument3 pagesHallucinations NCP PDFANGELA ERES BALINGBING100% (2)
- ASSESSMENTDocument3 pagesASSESSMENTJhenia Mae EulbNo ratings yet
- Nursing Care Plan For Mr. John E: Assessment Diagnosis Planning Intervention Rational EvaluationDocument1 pageNursing Care Plan For Mr. John E: Assessment Diagnosis Planning Intervention Rational EvaluationArnold Dickens JosephNo ratings yet
- NCP1Document4 pagesNCP1ejyoung928No ratings yet
- Nursing Care Plan of Disturbed Thought Process: Subjective Cues: General Objectives: Independent InterventionDocument15 pagesNursing Care Plan of Disturbed Thought Process: Subjective Cues: General Objectives: Independent InterventionJanella JinksonNo ratings yet
- College of Health Sciences: Urdaneta City UniversityDocument2 pagesCollege of Health Sciences: Urdaneta City UniversityDan Dan ManaoisNo ratings yet
- NCP TikDocument4 pagesNCP Tikblancher erNo ratings yet
- Assessment Diagnosis Planning Goal Implementation Rationale EvaluationDocument5 pagesAssessment Diagnosis Planning Goal Implementation Rationale EvaluationFatima C. Malik3181323No ratings yet
- Nursing Care Plan 1Document3 pagesNursing Care Plan 1Kuro HanabusaNo ratings yet
- NCP MentalDocument3 pagesNCP MentalColleen De la RosaNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument7 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationMaria Fatima MagsinoNo ratings yet
- NCPDocument3 pagesNCPCeeNo ratings yet
- NCP Fear PDF Relaxation (Psychology) Positive Psychology 2Document1 pageNCP Fear PDF Relaxation (Psychology) Positive Psychology 2BERSAMERA JOVEN 1CNo ratings yet
- Nursing Care Plan Submitted By: Kristian Dave DivaDocument11 pagesNursing Care Plan Submitted By: Kristian Dave DivaKristian Dave DivaNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument10 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationVincent PolicarNo ratings yet
- Date Identified: July 13, 2021 Date Evaluated: July 20, 2021 TetengDocument5 pagesDate Identified: July 13, 2021 Date Evaluated: July 20, 2021 Tetengkuro hanabusaNo ratings yet
- Aaa Gastrectomy NCP FinalDocument13 pagesAaa Gastrectomy NCP Finallexzaf100% (1)
- NCP Anxiety DRDocument3 pagesNCP Anxiety DRyuri dominxNo ratings yet
- Mokalid, Bkom NCPDocument7 pagesMokalid, Bkom NCPKC Olaizzah MokalidNo ratings yet
- Psychological Adaptations in PostpartumDocument7 pagesPsychological Adaptations in PostpartumKristine JamilleNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationJonna Mae TurquezaNo ratings yet
- 3nu04 - Group 4 - NCPDocument16 pages3nu04 - Group 4 - NCPKate Bianca GofredoNo ratings yet
- NCP-Disturbed Thought Process Related To Panic Level of AnxietyDocument1 pageNCP-Disturbed Thought Process Related To Panic Level of AnxietyopxNo ratings yet
- How To Use Your Subconscious Mind To Remove Fear - Based On The Teachings Of Dr. Joseph Murphy: Conquering Fear From WithinFrom EverandHow To Use Your Subconscious Mind To Remove Fear - Based On The Teachings Of Dr. Joseph Murphy: Conquering Fear From WithinNo ratings yet
- Gi Notes Lam The BestDocument6 pagesGi Notes Lam The BestIngrid Valerie BalendezNo ratings yet
- Seatwork 115Document2 pagesSeatwork 115Ingrid Valerie BalendezNo ratings yet
- READING ASSIGNMENT #1: Defining History by Robert Milton Underwood JRDocument2 pagesREADING ASSIGNMENT #1: Defining History by Robert Milton Underwood JRIngrid Valerie BalendezNo ratings yet
- Attributes of God: I. Omnipotence and Perfect GoodnessDocument7 pagesAttributes of God: I. Omnipotence and Perfect GoodnessIngrid Valerie BalendezNo ratings yet
- FLEX ELEARN - Online Course Teaching and Learning Agreement FormDocument1 pageFLEX ELEARN - Online Course Teaching and Learning Agreement FormLARS CUSSACK CONSAD SEPENo ratings yet
- DefiningHistory PDFDocument10 pagesDefiningHistory PDFOguzhan DonmezNo ratings yet
- Duty Requirements: in Partial Fulfillment of The Requirements For The Subject NCM 116Document10 pagesDuty Requirements: in Partial Fulfillment of The Requirements For The Subject NCM 116Ingrid Valerie BalendezNo ratings yet
- What I Like British English StudentDocument7 pagesWhat I Like British English StudentIngrid Valerie BalendezNo ratings yet
- Subject: Dr. Professor - Month YearDocument2 pagesSubject: Dr. Professor - Month YearCamila BarzagaNo ratings yet
- Level 4 Long Tests and Major Exam GuidelinesDocument1 pageLevel 4 Long Tests and Major Exam GuidelinesIngrid Valerie BalendezNo ratings yet
- Ingrid Valerie Roxas Balendez - Task 1 For English 65 NBDocument2 pagesIngrid Valerie Roxas Balendez - Task 1 For English 65 NBIngrid Valerie BalendezNo ratings yet
- Prokes Bahasa Inggris StuntingDocument15 pagesProkes Bahasa Inggris StuntingKameliaNo ratings yet
- Presentations Day 1 - Session 1 - Presentation 06 - Sri LankaDocument29 pagesPresentations Day 1 - Session 1 - Presentation 06 - Sri LankaAnkur MishraNo ratings yet
- (OSHPD 1, 2, 3 & 4) See Sections 404.0 Through 418.0. (SFM) Air Filters Shall Comply With All Requirements ofDocument0 pages(OSHPD 1, 2, 3 & 4) See Sections 404.0 Through 418.0. (SFM) Air Filters Shall Comply With All Requirements ofOanh NguyenNo ratings yet
- CrimPro Cases (Rule 116)Document45 pagesCrimPro Cases (Rule 116)elvinperiaNo ratings yet
- A Chance To Save Millions of Lives by Freeing Up Drug Patents - Advanced PDFDocument5 pagesA Chance To Save Millions of Lives by Freeing Up Drug Patents - Advanced PDFhahahapsuNo ratings yet
- A Decade of Dementia Care Training Learning Needs PDFDocument10 pagesA Decade of Dementia Care Training Learning Needs PDFYovana Pachón PovedaNo ratings yet
- Inspection ReportDocument5 pagesInspection ReportVimal SinghNo ratings yet
- WCLC2017 Abstract Book WebDocument700 pagesWCLC2017 Abstract Book Webdavid.yb.wangNo ratings yet
- Ims 1 10 18Document2 pagesIms 1 10 18Katherine UrregoNo ratings yet
- Acetic AnhydrideDocument8 pagesAcetic AnhydrideAsyraf SabriNo ratings yet
- Therapeutic PhlebotomyDocument2 pagesTherapeutic PhlebotomyAimee Howle BuchananNo ratings yet
- 2015annualreport 1Document46 pages2015annualreport 1Kathryn Jan DomingoNo ratings yet
- Bahasa Inggris Swot Madam Gie Sweet Cheek BlushedDocument8 pagesBahasa Inggris Swot Madam Gie Sweet Cheek Blushedanon_681594518No ratings yet
- Direct Black 22Document4 pagesDirect Black 22DHRUVNo ratings yet
- Common Skin Diseases in Africa: An Illustrated GuideDocument85 pagesCommon Skin Diseases in Africa: An Illustrated GuideJohn EnioladeNo ratings yet
- Abnormal Illness BehaviorDocument7 pagesAbnormal Illness Behavioransha2011p0% (1)
- Comparison of Intraocular Pressure After Water Drinking Test in Primary Open Angle Glaucoma Patients Controlled With Latanoprost and TrabeculectomyDocument7 pagesComparison of Intraocular Pressure After Water Drinking Test in Primary Open Angle Glaucoma Patients Controlled With Latanoprost and TrabeculectomyDimas Djiwa DNo ratings yet
- Xcelera Brochure Updated (English)Document24 pagesXcelera Brochure Updated (English)Pablo Rosas100% (1)
- MSDS Cim PremixDocument3 pagesMSDS Cim PremixKiệt Lê TuấnNo ratings yet
- Presentation On PDSDocument14 pagesPresentation On PDSShiva TantiNo ratings yet
- Influence of Potassium Sulfate On Faba Bean Yield and QualityDocument9 pagesInfluence of Potassium Sulfate On Faba Bean Yield and QualityMoehammad AlqamariNo ratings yet
- Jonsen 4 Box MethodDocument5 pagesJonsen 4 Box MethodsawsanNo ratings yet