You might also like
- Cerebral Herniation Syndromes and Intracranial HypertensionFrom EverandCerebral Herniation Syndromes and Intracranial HypertensionMatthew KoenigNo ratings yet
- "Mayroong Namuong Dugo Sa Utak Niya Kaya Hindi Maayos Ang Daloy NG Dugo Rito" As Verbalized by The Patient'sDocument4 pages"Mayroong Namuong Dugo Sa Utak Niya Kaya Hindi Maayos Ang Daloy NG Dugo Rito" As Verbalized by The Patient'sAllisson BeckersNo ratings yet
- (-1) PE ASTA O CITESTI PRIMA José Biller-Practical Neurology-LWW (2017) PDFDocument1,470 pages(-1) PE ASTA O CITESTI PRIMA José Biller-Practical Neurology-LWW (2017) PDFDutaCristianNo ratings yet
- 852-Article Text-1602-1-10-20190613Document12 pages852-Article Text-1602-1-10-20190613anidar1245No ratings yet
- Double-Outlet Left Ventricle and Vascular MalformationsDocument3 pagesDouble-Outlet Left Ventricle and Vascular MalformationsRaul UrietaNo ratings yet
- Posterior Reversible Encephalopathy Syndrome Secondary To Acute Post-Streptococcal Glomerulonephritis in A 12-Year-Old GirlDocument2 pagesPosterior Reversible Encephalopathy Syndrome Secondary To Acute Post-Streptococcal Glomerulonephritis in A 12-Year-Old GirlwawaningNo ratings yet
- Adem LikeDocument4 pagesAdem LikeRodrigo AriasNo ratings yet
- Electrocardiographic Changes and Intracranial Pathology: Geraldine Syverud, Crna, BSNDocument4 pagesElectrocardiographic Changes and Intracranial Pathology: Geraldine Syverud, Crna, BSNchuck55No ratings yet
- Angioinvasive Cerebral Aspergillosis Presenting As Acute Ischaemic Stroke in A Patient With Diabetes MellitusDocument4 pagesAngioinvasive Cerebral Aspergillosis Presenting As Acute Ischaemic Stroke in A Patient With Diabetes MellitusKamil HannaNo ratings yet
- 1 PBDocument3 pages1 PBYudith Paula MonicaNo ratings yet
- Exercise-Associated Numbness and Tingling in The Legs: For Editorial Comment See Page 1509Document4 pagesExercise-Associated Numbness and Tingling in The Legs: For Editorial Comment See Page 1509herpthederpNo ratings yet
- BCR 2012 007205Document4 pagesBCR 2012 007205shofidhiaaaNo ratings yet
- Research On Post Reversible Encephalopathy Due To Blood TransfusionsDocument7 pagesResearch On Post Reversible Encephalopathy Due To Blood TransfusionsAnkit AgarwalNo ratings yet
- Ipsilateral Hemiparesis and Contralateral Lower Limb Paresis Caused by Anterior Cerebral Artery Territory InfarctDocument4 pagesIpsilateral Hemiparesis and Contralateral Lower Limb Paresis Caused by Anterior Cerebral Artery Territory InfarctWati israNo ratings yet
- E110 FullDocument2 pagesE110 FullLuther ThengNo ratings yet
- Survival of A Neurologically Intact Patient With Subarachnoid Hemorrhage and Cardiopulmonary ArrestDocument4 pagesSurvival of A Neurologically Intact Patient With Subarachnoid Hemorrhage and Cardiopulmonary ArrestDino RatnamNo ratings yet
- Decreased Consciousness Bithalamic InfarcDocument3 pagesDecreased Consciousness Bithalamic InfarcshofidhiaaaNo ratings yet
- NurologyDocument3 pagesNurologytorosvartaniantorosNo ratings yet
- Cefalea Por Hipotension Complicada Con Herniacion Central Por Hematomas SubduralesDocument7 pagesCefalea Por Hipotension Complicada Con Herniacion Central Por Hematomas SubduralesFarid Santiago Abedrabbo LombeydaNo ratings yet
- Central Variant PRESDocument5 pagesCentral Variant PRESAbdul AzeezNo ratings yet
- Osmotic Demyelination Syndrome.Document5 pagesOsmotic Demyelination Syndrome.Nontaphon PiyawattanamethaNo ratings yet
- Acute Pseudobulbar Palsy After Bilateral ParamediaDocument6 pagesAcute Pseudobulbar Palsy After Bilateral ParamediaGeraldi ContrerasNo ratings yet
- Cortical Laminar NecrosisDocument7 pagesCortical Laminar Necrosisbalajinagarajanas2001No ratings yet
- BH 010060 ENGDocument2 pagesBH 010060 ENGCarlosNo ratings yet
- The Dangers of PRESDocument5 pagesThe Dangers of PRESShahnaaz ShahNo ratings yet
- A Case of Deep Cerebral Venous Thrombosis Presenting Like Acute Necrotizing EncephalopathyDocument4 pagesA Case of Deep Cerebral Venous Thrombosis Presenting Like Acute Necrotizing EncephalopathySachin DangiNo ratings yet
- Cranial Neuropathies in Granulomatosis With PolyangiitisDocument6 pagesCranial Neuropathies in Granulomatosis With PolyangiitisMikeyNo ratings yet
- Siddiqui Et Al. - 2017 - World NeurosurgeryDocument16 pagesSiddiqui Et Al. - 2017 - World NeurosurgeryubaidNo ratings yet
- RHS 2022Document3 pagesRHS 2022winnerfromparisNo ratings yet
- A 38 Year Old Woman With Global Aphasia and MigraiDocument4 pagesA 38 Year Old Woman With Global Aphasia and MigraiAchmad Dodi MeidiantoNo ratings yet
- Electrocardiographic Artifact MisleadiDocument5 pagesElectrocardiographic Artifact MisleadiMSNo ratings yet
- Acute Ischemic Stroke in Systemic Lupus Erythematosus: Challenges For Thrombolytic Therapy PDFDocument4 pagesAcute Ischemic Stroke in Systemic Lupus Erythematosus: Challenges For Thrombolytic Therapy PDFAshishsanjay MunoliNo ratings yet
- TTH Journal 4 PDFDocument5 pagesTTH Journal 4 PDFRumah Kost Kontrakan AntapaniNo ratings yet
- Teaching Neuroimages: Hemorrhagic Cavernoma With Secondary Development of Hypertrophic Olivary DegenerationDocument3 pagesTeaching Neuroimages: Hemorrhagic Cavernoma With Secondary Development of Hypertrophic Olivary DegenerationSamuel MorenoNo ratings yet
- MCQ Cardio 3Document50 pagesMCQ Cardio 3Dian ParamitaNo ratings yet
- Nonspecific Camel-Hump: SpecificDocument2 pagesNonspecific Camel-Hump: SpecificandreasgiannNo ratings yet
- Bilateral Acute Cerebellar InfarctsDocument3 pagesBilateral Acute Cerebellar InfarctsChandrashekhar SohoniNo ratings yet
- Part 1 CNS CasesDocument10 pagesPart 1 CNS CasesMicole NatividadNo ratings yet
- 33 PDFDocument3 pages33 PDFZeptalanNo ratings yet
- Corazon y SojenDocument7 pagesCorazon y Sojenmaria cristina aravenaNo ratings yet
- Laporan Kasus-Acute Embolic Stroke As The Sole Presentation of Infective Endocarditis in Mitral Valve ProlapseDocument2 pagesLaporan Kasus-Acute Embolic Stroke As The Sole Presentation of Infective Endocarditis in Mitral Valve ProlapseSari Novianty SilitongaNo ratings yet
- 2017 32 3 264 267 EngDocument4 pages2017 32 3 264 267 Engemmanuellagrace06No ratings yet
- Posterior Reversible Encephalopathy Syndrome After Lumbar PunctureDocument2 pagesPosterior Reversible Encephalopathy Syndrome After Lumbar PunctureMedtext PublicationsNo ratings yet
- Intracranial Hypertension As An Initial Clinical Manifestation of Systemic Lupus ErythematosusDocument11 pagesIntracranial Hypertension As An Initial Clinical Manifestation of Systemic Lupus Erythematosuszee zeeNo ratings yet
- A Case Report of Hydrocephalus in A US Military RecruitDocument3 pagesA Case Report of Hydrocephalus in A US Military RecruitRomita PutriNo ratings yet
- Overview of Imaging Modalities For Cerebral Aneurysms: Soroush Zaghi BIDMC PCE: Radiology August 2008Document26 pagesOverview of Imaging Modalities For Cerebral Aneurysms: Soroush Zaghi BIDMC PCE: Radiology August 2008Ardiansyah P PratamaNo ratings yet
- Hypoglycemia The Great Chameleon A Pseudo NonconDocument3 pagesHypoglycemia The Great Chameleon A Pseudo NonconuchoaNo ratings yet
- Lupus Myocarditis Presenting As Acute Congestive Heart FailureDocument3 pagesLupus Myocarditis Presenting As Acute Congestive Heart FailurehafifanisaNo ratings yet
- Inappropriate Sinus TachycardiaDocument23 pagesInappropriate Sinus TachycardiaOnon EssayedNo ratings yet
- Pons LesionDocument4 pagesPons Lesiontjimen2No ratings yet
- J Clinph 2013 03 031Document7 pagesJ Clinph 2013 03 031Andres Rojas JerezNo ratings yet
- Grand Case: Submitted ToDocument67 pagesGrand Case: Submitted ToPam Romero0% (1)
- Moya Sy 2 ChildrenDocument11 pagesMoya Sy 2 Childrenthomsoon01No ratings yet
- Case Study StrokeDocument5 pagesCase Study StrokelilutzuNo ratings yet
- Lee 2015Document12 pagesLee 2015Bagus Pithu Ha SpingNo ratings yet
- Crochetage Sign: An Invaluable Independent ECG Sign in Detecting ASDDocument2 pagesCrochetage Sign: An Invaluable Independent ECG Sign in Detecting ASDRicardanteNo ratings yet
- Raised Intracranial PressureDocument6 pagesRaised Intracranial PressureindihimmakhairaniNo ratings yet
- Clinical Reasoning: A Young Man With Recurrent Paralysis, Revisable White Matter Lesions and Peripheral Neuropathy Word Count: 945Document13 pagesClinical Reasoning: A Young Man With Recurrent Paralysis, Revisable White Matter Lesions and Peripheral Neuropathy Word Count: 945aileenzhongNo ratings yet
- J Neurol Neurosurg Psychiatry 2002 Dunn I23 7Document6 pagesJ Neurol Neurosurg Psychiatry 2002 Dunn I23 7milky1792No ratings yet
- Report of Cold Agglutinins in A Patient With Acute Ischemic StrokeDocument3 pagesReport of Cold Agglutinins in A Patient With Acute Ischemic StrokenovaNo ratings yet
- KCJ 42 568Document3 pagesKCJ 42 568vam buddhaNo ratings yet
- Massive Pulmonary Embolism Presenting As Seizures: December 2008 Vol 10 No 4Document4 pagesMassive Pulmonary Embolism Presenting As Seizures: December 2008 Vol 10 No 4BelladonnaRoxNo ratings yet
- Association Between Mentally Stimulating ActivitiesDocument7 pagesAssociation Between Mentally Stimulating ActivitiesAlvaro Martinez TorresNo ratings yet
- International Journal of Infectious Diseases: Lists Available atDocument9 pagesInternational Journal of Infectious Diseases: Lists Available atindanazulfaaNo ratings yet
- Counseling About Sudden Unexpected Death in Epilepsy (SUDEP)Document7 pagesCounseling About Sudden Unexpected Death in Epilepsy (SUDEP)indanazulfaaNo ratings yet
- Risk of Seizure Recurrence From Antiepileptic Drug WithdrawalDocument6 pagesRisk of Seizure Recurrence From Antiepileptic Drug WithdrawalindanazulfaaNo ratings yet
- Efficacy of Levetiracetam, Fosphenytoin, and Valproate For Established Status Epilepticus by Age Group (ESETT) : A Double-Blind, Responsive-Adaptive, Randomised Controlled TrialDocument8 pagesEfficacy of Levetiracetam, Fosphenytoin, and Valproate For Established Status Epilepticus by Age Group (ESETT) : A Double-Blind, Responsive-Adaptive, Randomised Controlled TrialEva FadilaNo ratings yet
- Neuroscience and Biobehavioral ReviewsDocument13 pagesNeuroscience and Biobehavioral ReviewsindanazulfaaNo ratings yet
- Effect of Acetylcholinesterase Inhibitors On Post-Stroke Cognitive Impairment and Vascular Dementia: A Meta-AnalysisDocument10 pagesEffect of Acetylcholinesterase Inhibitors On Post-Stroke Cognitive Impairment and Vascular Dementia: A Meta-AnalysisindanazulfaaNo ratings yet
- Neurochemistry International: Satoshi Hosoki, Tomotaka Tanaka, Masafumi IharaDocument9 pagesNeurochemistry International: Satoshi Hosoki, Tomotaka Tanaka, Masafumi IharaindanazulfaaNo ratings yet
- Archives of Gerontology and GeriatricsDocument6 pagesArchives of Gerontology and GeriatricsindanazulfaaNo ratings yet
- Function-Based Dementia Severity Assessment For Vascular Cognitive ImpairmentDocument9 pagesFunction-Based Dementia Severity Assessment For Vascular Cognitive ImpairmentindanazulfaaNo ratings yet
- Journal of The Neurological SciencesDocument7 pagesJournal of The Neurological SciencesindanazulfaaNo ratings yet
- Effect of Acetylcholinesterase Inhibitors On Post-Stroke Cognitive Impairment and Vascular Dementia: A Meta-AnalysisDocument10 pagesEffect of Acetylcholinesterase Inhibitors On Post-Stroke Cognitive Impairment and Vascular Dementia: A Meta-AnalysisindanazulfaaNo ratings yet
- Clinical Efficacy and Safety of Donepezil in The Treatment of Alzheimer's Disease in Chinese PatientsDocument8 pagesClinical Efficacy and Safety of Donepezil in The Treatment of Alzheimer's Disease in Chinese PatientsindanazulfaaNo ratings yet
- Siba Bre GeeDocument13 pagesSiba Bre GeeindanazulfaaNo ratings yet
- Raafi Haidar Arrasyid, Endah Sari Ratna Kumala, Nisrina Hanifah AfnanDocument10 pagesRaafi Haidar Arrasyid, Endah Sari Ratna Kumala, Nisrina Hanifah AfnanindanazulfaaNo ratings yet
- Cerebral Microvascular and Microstructural Integrity Is Regionally Altered in Patients With Systemic Lupus ErythematosusDocument9 pagesCerebral Microvascular and Microstructural Integrity Is Regionally Altered in Patients With Systemic Lupus ErythematosusindanazulfaaNo ratings yet
- Case Report Pons 2Document3 pagesCase Report Pons 2indanazulfaaNo ratings yet
- Intracranial Large Artery Abnormalities and Association With Cerebral Small Vessel Disease in CADASILDocument8 pagesIntracranial Large Artery Abnormalities and Association With Cerebral Small Vessel Disease in CADASILindanazulfaaNo ratings yet
- Severe Impairment Battery Language ScaleDocument5 pagesSevere Impairment Battery Language ScaleindanazulfaaNo ratings yet
- Case Report Pons 4Document4 pagesCase Report Pons 4indanazulfaaNo ratings yet
- Faktor Prognosis PonsDocument9 pagesFaktor Prognosis PonsindanazulfaaNo ratings yet
- Guide Line Lupus 2019Document10 pagesGuide Line Lupus 2019Anonymous 7dsX2F8nNo ratings yet
- Guide Line Lupus 2019Document10 pagesGuide Line Lupus 2019Anonymous 7dsX2F8nNo ratings yet
- Intracranial Arterial Stenosis Associated With Hashimoto's Disease Angiographic Features and Clinical OutcomesDocument8 pagesIntracranial Arterial Stenosis Associated With Hashimoto's Disease Angiographic Features and Clinical OutcomesindanazulfaaNo ratings yet
- COVID-19 and Cerebrovascular Diseases A Systematic Review and Perspectives For Stroke ManagementDocument14 pagesCOVID-19 and Cerebrovascular Diseases A Systematic Review and Perspectives For Stroke ManagementindanazulfaaNo ratings yet
- Intracranial Large Artery Abnormalities and Association With Cerebral Small Vessel Disease in CADASILDocument8 pagesIntracranial Large Artery Abnormalities and Association With Cerebral Small Vessel Disease in CADASILindanazulfaaNo ratings yet
- Cerebral Microvascular and Microstructural Integrity Is Regionally Altered in Patients With Systemic Lupus ErythematosusDocument9 pagesCerebral Microvascular and Microstructural Integrity Is Regionally Altered in Patients With Systemic Lupus ErythematosusindanazulfaaNo ratings yet
- Intracranial Arterial Stenosis Associated With Hashimoto's Disease Angiographic Features and Clinical OutcomesDocument8 pagesIntracranial Arterial Stenosis Associated With Hashimoto's Disease Angiographic Features and Clinical OutcomesindanazulfaaNo ratings yet
- COVID-19 and Cerebrovascular Diseases A Systematic Review and Perspectives For Stroke ManagementDocument14 pagesCOVID-19 and Cerebrovascular Diseases A Systematic Review and Perspectives For Stroke ManagementindanazulfaaNo ratings yet
- High-Altitude MedicineDocument12 pagesHigh-Altitude MedicineSNo ratings yet
- Enhanced Proliferation of Visualizable Mesenchymal Stem Cell Platelet Hybrid Cell For Versatile Intracerebral Hemorrhage TreatmentDocument14 pagesEnhanced Proliferation of Visualizable Mesenchymal Stem Cell Platelet Hybrid Cell For Versatile Intracerebral Hemorrhage Treatment马三强No ratings yet
- Elevated Intracranial PressureDocument53 pagesElevated Intracranial PressureHandre PutraNo ratings yet
- Diabetic Ketoacidosis in ChildrenDocument6 pagesDiabetic Ketoacidosis in ChildrenviharadewiNo ratings yet
- Intracranial PressureDocument27 pagesIntracranial PressureAnggaSunaryaNo ratings yet
- Malignant Cerebral Hemispheric Infarction With Swelling and Risk of Herniation - UpToDateDocument31 pagesMalignant Cerebral Hemispheric Infarction With Swelling and Risk of Herniation - UpToDateFátima Gutiérrez ValdiviaNo ratings yet
- Medical Surgical Nursing 2 HighlightsDocument7 pagesMedical Surgical Nursing 2 HighlightsMatt Andrei P. SongcuanNo ratings yet
- Transient Ischemic Attack Precipitating Factors Predisposing FactorsDocument6 pagesTransient Ischemic Attack Precipitating Factors Predisposing FactorsYosef OxinioNo ratings yet
- Management of Acute Moderate and Severe Traumatic Brain Injury - UpToDateDocument80 pagesManagement of Acute Moderate and Severe Traumatic Brain Injury - UpToDateManuelEduardoSanchezSotoNo ratings yet
- Metabolic Encephalopathies in The Critical Care Unit: Review ArticleDocument29 pagesMetabolic Encephalopathies in The Critical Care Unit: Review ArticleFernando Dueñas MoralesNo ratings yet
- Ghost CapDocument4 pagesGhost Capmedico89No ratings yet
- m146 PDFDocument697 pagesm146 PDFspgoniNo ratings yet
- Nursing Care Plan On FeverDocument15 pagesNursing Care Plan On Feverkamini ChoudharyNo ratings yet
- 100Document14 pages100Mohammed BISHRNo ratings yet
- Clinical Relevance of Steroid Use in Neuro-Oncology. 2017Document10 pagesClinical Relevance of Steroid Use in Neuro-Oncology. 2017Nicolas RodriguezNo ratings yet
- Head InjuryDocument69 pagesHead Injuryheena solankiNo ratings yet
- Brain Tumor ICP Head and Neck CA TracheostomyDocument11 pagesBrain Tumor ICP Head and Neck CA TracheostomyWincy Faith SalazarNo ratings yet
- Acute Hospital Management of Pediatric Stroke 2022Document12 pagesAcute Hospital Management of Pediatric Stroke 2022Ciarol BorbonNo ratings yet
- Step LadderExpansive Cranioplasty Mathametical ModelDocument7 pagesStep LadderExpansive Cranioplasty Mathametical ModelDebashree SenguptaNo ratings yet
- Traumatic Brain Injuries: Assoc. Prof. Dr. Vicentiu M. SăceleanuDocument38 pagesTraumatic Brain Injuries: Assoc. Prof. Dr. Vicentiu M. SăceleanuAnna DianaNo ratings yet
- Haemorrhagic StrokeDocument11 pagesHaemorrhagic Strokelengkong100% (2)
- Orig 20 Art 202Document5 pagesOrig 20 Art 202Putri AprilianiNo ratings yet
- Neuro CCNDocument5 pagesNeuro CCNShy Dela PuertaNo ratings yet
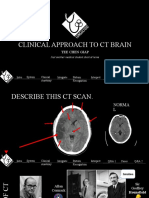
- Clinical Approach To CT BrainDocument34 pagesClinical Approach To CT BrainXiaoThoong LohNo ratings yet
- Fluid Therapy and Traumatic Brain Injury: A Narrative ReviewDocument6 pagesFluid Therapy and Traumatic Brain Injury: A Narrative ReviewmiguelalmenarezNo ratings yet
- CSF Shift Edema PublishedDocument15 pagesCSF Shift Edema PublishedIype CherianNo ratings yet
- Jurnal Kad Dan HonkDocument9 pagesJurnal Kad Dan Honksimpati91No ratings yet
- Only Use If 2.7% Polyfusor Unavailable: Remove 36mls 0.9% Saline Add 36mls 30% SalineDocument1 pageOnly Use If 2.7% Polyfusor Unavailable: Remove 36mls 0.9% Saline Add 36mls 30% SalineBlessing NdlovuNo ratings yet