You might also like
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- Helminths MCQsDocument21 pagesHelminths MCQsمحمد محمد هشام83% (18)
- Broad Spectrum AntibioticsDocument17 pagesBroad Spectrum AntibioticsRabi ShahNo ratings yet
- Tetracyclines ChloramphenicolDocument32 pagesTetracyclines ChloramphenicolBishal ChauhanNo ratings yet
- Broad Broad Spectrum Antibiotics Spectrum Antibiotics Spectrum Antibiotics Spectrum AntibioticsDocument41 pagesBroad Broad Spectrum Antibiotics Spectrum Antibiotics Spectrum Antibiotics Spectrum AntibioticsAmit HaldarNo ratings yet
- Protein Synthesis InhibitorsDocument173 pagesProtein Synthesis InhibitorsAssssssNo ratings yet
- TetracylinesDocument17 pagesTetracylinesPhoenixNo ratings yet
- EIGBEFOH Pharmacology of AntimicrobialsDocument59 pagesEIGBEFOH Pharmacology of AntimicrobialskbNo ratings yet
- Anti-Infective PPDocument30 pagesAnti-Infective PPHlaSoe WinNo ratings yet
- Tetracycline's: Jagir R. Patel Asst Prof Dept. Pharmacology Anand Pharmacy CollegeDocument21 pagesTetracycline's: Jagir R. Patel Asst Prof Dept. Pharmacology Anand Pharmacy CollegeJagirNo ratings yet
- 30.IndustrialMicrobiology 102008 105579Document32 pages30.IndustrialMicrobiology 102008 105579Asif IqbalNo ratings yet
- 44 Chloramphenicol, Tetracyclines, Macrolides, ClindamycinDocument77 pages44 Chloramphenicol, Tetracyclines, Macrolides, ClindamycinNagu KopparapuNo ratings yet
- Tetracycline Drug Reporting-2Document21 pagesTetracycline Drug Reporting-2Shynne RPhNo ratings yet
- Antibiotik Dan Antiseptik Saluran KemihDocument29 pagesAntibiotik Dan Antiseptik Saluran KemihPutri Sari SeptirianiNo ratings yet
- Antimicrobial DrugsDocument63 pagesAntimicrobial DrugsMarianaBologanNo ratings yet
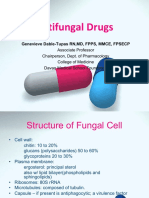
- Antifungal Drugs (Revised) Aug 2022Document62 pagesAntifungal Drugs (Revised) Aug 2022sankethNo ratings yet
- Class 10 Tetracyclins and AmphenicolsDocument35 pagesClass 10 Tetracyclins and AmphenicolsSangeetha KannanNo ratings yet
- Antifungal PharamcotherapyDocument29 pagesAntifungal Pharamcotherapyrijay2001No ratings yet
- Acute Infectious Diarrheal Diseases and Bacterial Food PoisoningDocument32 pagesAcute Infectious Diarrheal Diseases and Bacterial Food PoisoningVenkatesh GarikapatiNo ratings yet
- Common Antibiotics Master ListDocument20 pagesCommon Antibiotics Master ListMahendra VermaNo ratings yet
- Tetracycline Antibiotics GuideDocument9 pagesTetracycline Antibiotics Guideedle maeNo ratings yet
- Anti-Protozoal Drugs: Dr. Mozna TalpurDocument25 pagesAnti-Protozoal Drugs: Dr. Mozna TalpurShahid Hameed100% (1)
- Kuliah Antihelmintic DrugsDocument23 pagesKuliah Antihelmintic DrugsBaiqLinaAnggrianNo ratings yet
- Pharmacology of AntibioticDocument66 pagesPharmacology of AntibioticfgrehNo ratings yet
- Antibiotics: Faculty of Dentistry 22 September 2014Document61 pagesAntibiotics: Faculty of Dentistry 22 September 2014gamalsolimanNo ratings yet
- MACROLIDESDocument51 pagesMACROLIDESKasturiRangan SrivatsaNo ratings yet
- 44-45 Tetracyclines and Chloramphenicols-2023Document30 pages44-45 Tetracyclines and Chloramphenicols-2023deo okiaNo ratings yet
- Chloramphenicol: Prof DR Shah Murad 0314-2243415Document47 pagesChloramphenicol: Prof DR Shah Murad 0314-2243415PROF DR SHAHMURADNo ratings yet
- Reviewer - Pharmacology FinalsDocument17 pagesReviewer - Pharmacology Finalsarmanuel1390antNo ratings yet
- 83017809-Tetracyclines-Medicinal ChemistryDocument40 pages83017809-Tetracyclines-Medicinal ChemistryKevin Chapley100% (1)
- ANTIFUNGAL AGENTS: A REVIEWDocument24 pagesANTIFUNGAL AGENTS: A REVIEWfitri dwiyantiNo ratings yet
- ChloramphenicolDocument20 pagesChloramphenicolPROF DR SHAHMURAD100% (2)
- AntibacterialsDocument8 pagesAntibacterialslisalynnleeNo ratings yet
- ANTIFUNGAL AGENTS FOR FUNGAL INFECTIONSDocument24 pagesANTIFUNGAL AGENTS FOR FUNGAL INFECTIONSBaiqLinaAnggrianNo ratings yet
- Anti Fungal & Anthelminthic DrugsDocument62 pagesAnti Fungal & Anthelminthic DrugsKasturiRangan SrivatsaNo ratings yet
- Antifungal DrugsDocument45 pagesAntifungal DrugsAbdulai WakoNo ratings yet
- 4 AntibiotikDocument85 pages4 AntibiotikDion Leonardo SiregarNo ratings yet
- Staphylococci: Major Pathogens and Disease ManifestationsDocument21 pagesStaphylococci: Major Pathogens and Disease ManifestationsAhmad Al ShdefatNo ratings yet
- Aminoglycosides: Dr. Amit ShahDocument29 pagesAminoglycosides: Dr. Amit ShahAmit ShahNo ratings yet
- Pharmacology - AntibacterialDocument46 pagesPharmacology - Antibacterialmanilyn100% (1)
- Protein Synthesis InhibitorsDocument28 pagesProtein Synthesis InhibitorsMaha JabeenNo ratings yet
- Protein Synthesis InhibitorsDocument6 pagesProtein Synthesis InhibitorsVanessa HermioneNo ratings yet
- Antibiotics-2Document38 pagesAntibiotics-2Tommy ZeusNo ratings yet
- AnthelminticsDocument5 pagesAnthelminticsDrx Harish PatelNo ratings yet
- "Clinical Pharmacology of Antibacterial DrugsDocument44 pages"Clinical Pharmacology of Antibacterial DrugsLucas Victor AlmeidaNo ratings yet
- Antibiotics:: Sulfonamides Penicillins Cephalosporins Tetracyclines Aminoglycosides Quinolones MacrolidesDocument67 pagesAntibiotics:: Sulfonamides Penicillins Cephalosporins Tetracyclines Aminoglycosides Quinolones MacrolidesMarcky_467100% (7)
- 4 Tetracyclines+ChloroamphDocument6 pages4 Tetracyclines+ChloroamphNashat SaadiNo ratings yet
- Microbial Diseases of The Digestive SystemDocument42 pagesMicrobial Diseases of The Digestive SystemAbhishek Isaac MathewNo ratings yet
- Antimicrobial Agents 2021Document82 pagesAntimicrobial Agents 2021Aprilene Angel Balaque ZunegaNo ratings yet
- Antibacterials, Antifungals and Antiparasitics: Mechanisms and Nursing ConsiderationsDocument10 pagesAntibacterials, Antifungals and Antiparasitics: Mechanisms and Nursing ConsiderationsKathleen MontañoNo ratings yet
- Antimikroba Dan Anti Alergi Topical-Dharma2018Document43 pagesAntimikroba Dan Anti Alergi Topical-Dharma2018Laras OktavianiNo ratings yet
- Antibiotik dan antiseptik saluran kemihDocument23 pagesAntibiotik dan antiseptik saluran kemihruuweelscribdNo ratings yet
- Antibiotics in Pediatrics (Vancomycin, Quinolones, Aminoglycosides, Tetracyclines, Chloramphenicol, Clindamycin, Macrolides)Document90 pagesAntibiotics in Pediatrics (Vancomycin, Quinolones, Aminoglycosides, Tetracyclines, Chloramphenicol, Clindamycin, Macrolides)Jill PNo ratings yet
- SULFONAMIDES Dr. NeenuDocument37 pagesSULFONAMIDES Dr. Neenuneenu csNo ratings yet
- Bovine MastitisDocument31 pagesBovine MastitisMitao WilbertNo ratings yet
- Antimycotic Agents and Their Properties: BY Mawuli Atiemo Central University College, AccraDocument25 pagesAntimycotic Agents and Their Properties: BY Mawuli Atiemo Central University College, AccraMawuli AtiemoNo ratings yet
- ANTIBIOTICSDocument51 pagesANTIBIOTICSamrharidi446No ratings yet
- Concise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryFrom EverandConcise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryNo ratings yet
- Percutaneous Transhepatic CholangiographyDocument3 pagesPercutaneous Transhepatic CholangiographyRonel UsitaNo ratings yet
- Module14 Content Nursing Care Management of AdultDocument21 pagesModule14 Content Nursing Care Management of AdultFranceska AntonioNo ratings yet
- Rebuilding The Food PyramidDocument6 pagesRebuilding The Food PyramidXenita Vera Lataza PitosNo ratings yet
- History and Development of MicrobiologyDocument9 pagesHistory and Development of Microbiologybetu8137No ratings yet
- Cue Problem Scientific Explanation Planning Interventions Rationale EvaluationDocument5 pagesCue Problem Scientific Explanation Planning Interventions Rationale EvaluationJanyn Abella ReyesNo ratings yet
- Chapter 28 PROMDocument24 pagesChapter 28 PROMTansya PurnaningrumNo ratings yet
- STOMATITISDocument17 pagesSTOMATITISTeguh Adi PartamaNo ratings yet
- Tube GuideDocument1 pageTube Guidezalam55No ratings yet
- OSH State University Microbiology Course Covers Bacteria, Viruses & ImmunityDocument15 pagesOSH State University Microbiology Course Covers Bacteria, Viruses & ImmunityKunal BhamareNo ratings yet
- Case 2 The FluDocument2 pagesCase 2 The FluJolo CutaranNo ratings yet
- MOnonucleosis Patients InfoDocument2 pagesMOnonucleosis Patients Infoluisramos316No ratings yet
- Bioterrorism: BY: - Bijay Kumar Mahato BPH 2 Semester Padmashree School of Public HealthDocument26 pagesBioterrorism: BY: - Bijay Kumar Mahato BPH 2 Semester Padmashree School of Public HealthBijay Kumar MahatoNo ratings yet
- Intra Uterin Fetal DeathDocument15 pagesIntra Uterin Fetal DeathanojanNo ratings yet
- Garcinia Kola ThesisDocument36 pagesGarcinia Kola ThesisDdn RmaNo ratings yet
- Q SofaDocument9 pagesQ SofadarlingcarvajalduqueNo ratings yet
- COVID-19 Quiz Review for Nurses: Coronavirus Symptoms, Transmission & PreventionDocument11 pagesCOVID-19 Quiz Review for Nurses: Coronavirus Symptoms, Transmission & Preventionhasan ahmdNo ratings yet
- Ceftozolone TazobactamDocument12 pagesCeftozolone TazobactamMarisol ToribioNo ratings yet
- Health Benefits of Geranium Essential OilDocument2 pagesHealth Benefits of Geranium Essential OilMolibeli LibetsoNo ratings yet
- DNA ReplicationDocument44 pagesDNA ReplicationRana AttiqNo ratings yet
- Therapeutic Strategies in CopdDocument378 pagesTherapeutic Strategies in Copdgermany23No ratings yet
- Risk Factors For Celiac DiseaseDocument5 pagesRisk Factors For Celiac DiseaseMavili OcalNo ratings yet
- Clinical Flow Cytometry - Emerging ApplicationsDocument215 pagesClinical Flow Cytometry - Emerging ApplicationsDaoud IssaNo ratings yet
- Para Notes - SummaryDocument4 pagesPara Notes - SummaryReg LagartejaNo ratings yet
- Tinea KorporisDocument3 pagesTinea Korporishaprisia winaNo ratings yet
- Clinical Pharmacokinetics in Liver Failure Patients SenddDocument30 pagesClinical Pharmacokinetics in Liver Failure Patients Senddthavia andrianiNo ratings yet
- Antimicrobial AgentDocument46 pagesAntimicrobial Agentسامر الرفاعيNo ratings yet
- Diarrhea (Diare)Document9 pagesDiarrhea (Diare)Eki MegaraniNo ratings yet
- Diasorin Company Presentation Eng March 2022 1Document13 pagesDiasorin Company Presentation Eng March 2022 1Yaser MNo ratings yet
- CNS PathologyDocument10 pagesCNS Pathologysarguss1483% (6)