You might also like
- Angioplasty, (Stent Dilatation) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAngioplasty, (Stent Dilatation) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Equipment Devices and Procedures in The Intensive Care UnitDocument16 pagesEquipment Devices and Procedures in The Intensive Care UnitJade ParkNo ratings yet
- Topik 5. Reading Intensive Care UnitDocument33 pagesTopik 5. Reading Intensive Care UnitHabibiNo ratings yet
- Topik 4. Reading Intensive Care UnitDocument18 pagesTopik 4. Reading Intensive Care UnitioakasNo ratings yet
- Equipment Devices and Procedures in The Intensive Care Unit PDFDocument16 pagesEquipment Devices and Procedures in The Intensive Care Unit PDFJena Rose ReyesNo ratings yet
- Equipment You May See in The ICUDocument6 pagesEquipment You May See in The ICURaidis PangilinanNo ratings yet
- Equipment in The Intensive Care Unit - Eng Mohamed AliDocument8 pagesEquipment in The Intensive Care Unit - Eng Mohamed AliMohamed AliNo ratings yet
- Equipment, Devices, and Procedures in Intensive CareDocument12 pagesEquipment, Devices, and Procedures in Intensive CarepritasaNo ratings yet
- Icu OrientationDocument59 pagesIcu OrientationsethivanshikaNo ratings yet
- A. Cases of Patients Admitted in An ICU Generally, This Are The Few Common Condition of The Patients in ICUDocument5 pagesA. Cases of Patients Admitted in An ICU Generally, This Are The Few Common Condition of The Patients in ICUAngeline KimaykimayNo ratings yet
- Intensive Care UnitDocument6 pagesIntensive Care UnitPaula Delgadillo100% (1)
- Factsheet Common EquipmentDocument2 pagesFactsheet Common EquipmentRongalaSnehaNo ratings yet
- EQUIPMENTS in ICCUDocument5 pagesEQUIPMENTS in ICCUrhyanne100% (1)
- Mechanical Ventilation PDFDocument2 pagesMechanical Ventilation PDFSarahUtamiSr.No ratings yet
- Welcome TO Intensive Care UnitDocument42 pagesWelcome TO Intensive Care UnitKharene Lirazan100% (1)
- 2017 Mechanical VentilationDocument2 pages2017 Mechanical VentilationJose Luis Escobar zabaleguiNo ratings yet
- Monitoring Equipment in the ICUDocument5 pagesMonitoring Equipment in the ICUMon ManguilinNo ratings yet
- Subtypes of IcuDocument23 pagesSubtypes of IcuSrea AgnesNo ratings yet
- Guide to Endotracheal and Nasogastric Intubation ProceduresDocument9 pagesGuide to Endotracheal and Nasogastric Intubation ProceduresKate AbellaNo ratings yet
- First Aid AssignmentDocument14 pagesFirst Aid AssignmentJeremy Rei Mendroz100% (1)
- What Is Intubation? (Procedure, Study Guide, and Practice Questions)Document17 pagesWhat Is Intubation? (Procedure, Study Guide, and Practice Questions)Ching BanagNo ratings yet
- Thoracentesis: ProcedureDocument12 pagesThoracentesis: Procedurealbert manievoNo ratings yet
- Thoracentesis Reflective EssayDocument2 pagesThoracentesis Reflective EssayAnjae GariandoNo ratings yet
- What Is A Transjugular Intrahepatic Portosystemic Shunt (TIPS) ?Document7 pagesWhat Is A Transjugular Intrahepatic Portosystemic Shunt (TIPS) ?Tata Tamara Tam TamNo ratings yet
- tgs chelsa individu mr. bingsDocument4 pagestgs chelsa individu mr. bingsjeffriwahyudi91No ratings yet
- Thoracentesis Is Also Known As Pleural Fluid AnalysisDocument3 pagesThoracentesis Is Also Known As Pleural Fluid AnalysisJ.r. MercadoNo ratings yet
- ICU Procedure HandoutsDocument26 pagesICU Procedure HandoutsDadi Veen100% (2)
- Chest Tube Placement Dl1Document9 pagesChest Tube Placement Dl1Aziil LiizaNo ratings yet
- Learning About Icu Equipment: Adamson UniversityDocument5 pagesLearning About Icu Equipment: Adamson UniversityRaidis PangilinanNo ratings yet
- Emergency Laparotomy: Patient Information FactsheetDocument4 pagesEmergency Laparotomy: Patient Information FactsheetMuhammad RizqiNo ratings yet
- Et TubeDocument31 pagesEt Tubeinno so qtNo ratings yet
- Name: Kristella Marie C. Desiata Case AnalysisDocument2 pagesName: Kristella Marie C. Desiata Case AnalysisYamete KudasaiNo ratings yet
- SmmeryDocument2 pagesSmmeryIndriyaniiIntandewataNo ratings yet
- Critical Care Clinical Procedures 2023Document38 pagesCritical Care Clinical Procedures 2023nucahersheyskatNo ratings yet
- Nebulization Nursing Procedure at Ateneo de Zamboanga UniversityDocument9 pagesNebulization Nursing Procedure at Ateneo de Zamboanga UniversityMitzi BelamideNo ratings yet
- GUIDE OF INFORMATIONS REGARDING A PATIENT SUBMIT TO CORONARY ANGIOGRAM, ANGIOPLASTY AND STENT RV JBDocument9 pagesGUIDE OF INFORMATIONS REGARDING A PATIENT SUBMIT TO CORONARY ANGIOGRAM, ANGIOPLASTY AND STENT RV JBIsabel PauloNo ratings yet
- Tabije, Arvie Jayselle PDocument8 pagesTabije, Arvie Jayselle PJaysellePuguonTabijeNo ratings yet
- Surgical Bed Side ProceduressDocument62 pagesSurgical Bed Side Proceduressdrhiwaomer100% (1)
- Hemodialysis Shunt, Graft, and Fistula CareDocument11 pagesHemodialysis Shunt, Graft, and Fistula CareArjon Clint Reyes SulapasNo ratings yet
- 6.1 Cholecystectomy DazadesolocDocument23 pages6.1 Cholecystectomy DazadesolocMonette Abalos MendovaNo ratings yet
- VENTILATERSDocument12 pagesVENTILATERSDeekshith KumarNo ratings yet
- Comprehension TestDocument3 pagesComprehension TestMaryudha FirmansyahNo ratings yet
- Tracheostomy Training Resources: A Guide To Tracheostomy Management in Critical Care and BeyondDocument70 pagesTracheostomy Training Resources: A Guide To Tracheostomy Management in Critical Care and BeyondMarwah Alnoor YousufNo ratings yet
- IntubationDocument16 pagesIntubationSimina ÎntunericNo ratings yet
- What You Need To Know About Tracheostomy 2020Document10 pagesWhat You Need To Know About Tracheostomy 2020Agata KaczmarekNo ratings yet
- Chest Tube DrainageDocument3 pagesChest Tube DrainageCyndi Jane Bandin Cruzata100% (1)
- ThoracentesisDocument4 pagesThoracentesisCyntia Theresia Lumintang100% (1)
- Ccu NotesDocument76 pagesCcu NotesAr PeeNo ratings yet
- Perc Abscess DR NDocument5 pagesPerc Abscess DR NtgwesrgrdfNo ratings yet
- NIH Clinical Center Patient Education Materials: Transphenoidal SurgeryDocument4 pagesNIH Clinical Center Patient Education Materials: Transphenoidal SurgeryDapot Sianipar100% (1)
- Assisting For Endotracheal IntubationDocument16 pagesAssisting For Endotracheal IntubationSREEDEVI T SURESH100% (1)
- V. DhanajayanDocument9 pagesV. DhanajayanꜱᴀꜰɪᴇNo ratings yet
- THORACENTESISDocument11 pagesTHORACENTESISJeann sumbillaNo ratings yet
- HemodialysisDocument14 pagesHemodialysistri utamiNo ratings yet
- Cardiac Stent GuideDocument6 pagesCardiac Stent GuideAbrar KhafagaNo ratings yet
- Anesthetic Management: Hysterectomy: in This IssueDocument8 pagesAnesthetic Management: Hysterectomy: in This IssueTerrence ClemonsNo ratings yet
- Suctioning PDFDocument6 pagesSuctioning PDFIonel AfteneNo ratings yet
- Rules and Directions for the Employment of Injections in Various DiseasesFrom EverandRules and Directions for the Employment of Injections in Various DiseasesNo ratings yet
- Journal Titles and DetailsDocument30 pagesJournal Titles and DetailsMinerva Medical Treatment Pvt LtdNo ratings yet
- Esign IPS: Reducing Switching Losses in Portable DC/DC ConvertersDocument2 pagesEsign IPS: Reducing Switching Losses in Portable DC/DC ConvertersAbhishek SinghNo ratings yet
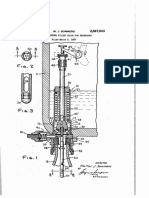
- Counter-pressure filler valve for beveragesDocument3 pagesCounter-pressure filler valve for beveragesbimalishaNo ratings yet
- PricelistDocument184 pagesPricelistWissam JarmakNo ratings yet
- SanCoP7 AgendaDocument2 pagesSanCoP7 AgendaNicolaGreeneNo ratings yet
- How To Judge A Dasha in JyotishDocument2 pagesHow To Judge A Dasha in JyotishRavan SharmaNo ratings yet
- RN and LPN Scope of Practice GuideDocument6 pagesRN and LPN Scope of Practice Guidejenn1722No ratings yet
- Solving Proportions Problems with Learning Activity SheetsDocument21 pagesSolving Proportions Problems with Learning Activity Sheetsceline fernandezNo ratings yet
- Strengthening HIV Care in Africa CertificateDocument7 pagesStrengthening HIV Care in Africa CertificateMaiga Ayub HusseinNo ratings yet
- Mitsubishi Galant 4g63 Engine Repair ManualDocument29 pagesMitsubishi Galant 4g63 Engine Repair ManualMoaed Kanbar100% (1)
- Sakshijain75.Final ProDocument46 pagesSakshijain75.Final ProOm AherNo ratings yet
- Economic Case for Immobilizing EnzymesDocument25 pagesEconomic Case for Immobilizing EnzymesNikki ChauhanNo ratings yet
- SEN Code of Practice 2001Document148 pagesSEN Code of Practice 2001Matt GrantNo ratings yet
- Dutch FarmDocument104 pagesDutch Farmdoc_abdullahNo ratings yet
- Land Tenure SystemsDocument140 pagesLand Tenure SystemsjoeclintNo ratings yet
- Gaggia Cadorna Milk Full Instruction ManualDocument76 pagesGaggia Cadorna Milk Full Instruction ManualKanen Coffee, LLC.No ratings yet
- Ramial Chipped Wood - A Basic Tool For Regenerating SoilsDocument15 pagesRamial Chipped Wood - A Basic Tool For Regenerating SoilsmrmiscNo ratings yet
- Healthy Lifestyle HabitsDocument2 pagesHealthy Lifestyle HabitsJesus BaldeonNo ratings yet
- Hector: Genuine AccessoriesDocument18 pagesHector: Genuine AccessoriesssgfdfgNo ratings yet
- General Conditions of Contracts For NLNG 2018Document28 pagesGeneral Conditions of Contracts For NLNG 2018AF Dowell MirinNo ratings yet
- EXU EN 2017-12 Manual Web PDFDocument126 pagesEXU EN 2017-12 Manual Web PDFИльнур ТагировNo ratings yet
- Different Surgical Modalities For Management of Postburn FL Exion Contracture of The ElbowDocument6 pagesDifferent Surgical Modalities For Management of Postburn FL Exion Contracture of The ElbowMadhuchandra HirehalliNo ratings yet
- Pathology AIIMSDocument26 pagesPathology AIIMSvkNo ratings yet
- NEOM-NDS-SPC-015 - 01.00 - Neutral Earthing Resistor (NER) SpecificationDocument15 pagesNEOM-NDS-SPC-015 - 01.00 - Neutral Earthing Resistor (NER) Specificationcawoc96196No ratings yet
- GMP TD Ar FPL 11033Document1 pageGMP TD Ar FPL 11033Sammy NguyenNo ratings yet
- Periodic Test in Tle - Grade Ix Electricity.Document2 pagesPeriodic Test in Tle - Grade Ix Electricity.Resneth MondejarNo ratings yet
- BiostastisticDocument2 pagesBiostastisticاحمد ماجد زبنNo ratings yet
- Apcosil 605Document1 pageApcosil 605rihtak123No ratings yet
- Starbucks BSC Project Analyzes Store PerformanceDocument8 pagesStarbucks BSC Project Analyzes Store Performanceandrea100% (1)
- The Prevention of Women & Children Repression Act 2000: A Study of Implementation Process From 2003 To 2013Document9 pagesThe Prevention of Women & Children Repression Act 2000: A Study of Implementation Process From 2003 To 2013Md. Abdul KarimNo ratings yet