You might also like
- Disability Attitudes in Health Care: A New Scale InstrumentDocument12 pagesDisability Attitudes in Health Care: A New Scale InstrumentLeila FortesNo ratings yet
- Undergraduate Medical Education: Attitude Change During Medical School: A Cohort StudyDocument13 pagesUndergraduate Medical Education: Attitude Change During Medical School: A Cohort StudyastriaciwidyaNo ratings yet
- Disaster Dan LansiaDocument9 pagesDisaster Dan Lansiaistianna nurhidayatiNo ratings yet
- Lynch 2019 - Understanding Disability' Evaluating A Contact-Based Approach To Enhance AtittudesDocument7 pagesLynch 2019 - Understanding Disability' Evaluating A Contact-Based Approach To Enhance AtittudesYerson Santiago PardoNo ratings yet
- A Review of Oppositional Defiant and Conduct DisordersDocument9 pagesA Review of Oppositional Defiant and Conduct DisordersStiven GonzalezNo ratings yet
- Ijnhs V7i2p102Document4 pagesIjnhs V7i2p102Seventh Sense Research GroupNo ratings yet
- NIH Public AccessDocument15 pagesNIH Public AccessSofía SciglianoNo ratings yet
- 1221 FullDocument6 pages1221 FulladrianesalikNo ratings yet
- 2012 AdolescentattitudesDocument7 pages2012 AdolescentattitudesMadawi AlotaibiNo ratings yet
- Psychology JournalDocument36 pagesPsychology JournalMarisa KwokNo ratings yet
- Attitudes Towards People With Mental IllnessDocument8 pagesAttitudes Towards People With Mental IllnessleticiaNo ratings yet
- Belief and AttitudeDocument10 pagesBelief and AttitudePreeti ChouhanNo ratings yet
- ED 303 Research No.3Document4 pagesED 303 Research No.3Cherry AduanNo ratings yet
- Attitude of Student Nurses' Toward People With DisabilitiesDocument48 pagesAttitude of Student Nurses' Toward People With DisabilitiesDaniel ObasiNo ratings yet
- Compte Et Al 2015, A Two-Stage Epidemiological Study of Eating Disorders and Muscle Dysmorphia in Male University Students in Buenos AiresDocument10 pagesCompte Et Al 2015, A Two-Stage Epidemiological Study of Eating Disorders and Muscle Dysmorphia in Male University Students in Buenos AiresEmilio J. CompteNo ratings yet
- Ehlers Danlos Syndrome PaperDocument6 pagesEhlers Danlos Syndrome Paperapi-611093731No ratings yet
- 2019 Addressing Sexuality Among People Living With Chronic Di 2020 Archives of PHDocument12 pages2019 Addressing Sexuality Among People Living With Chronic Di 2020 Archives of PHAngie OvandoNo ratings yet
- Gender Comparisons of Medical Students' Psychosocial Pro®lesDocument8 pagesGender Comparisons of Medical Students' Psychosocial Pro®lesRosyiidta JanahNo ratings yet
- Research PURCOMDocument2 pagesResearch PURCOMMaegan AzarconNo ratings yet
- Shashi Kumar 2014Document7 pagesShashi Kumar 2014SPE CommitteeNo ratings yet
- Literature Review Eating DisordersDocument12 pagesLiterature Review Eating Disordersafmzaoahmicfxg100% (1)
- Type A Type BDocument8 pagesType A Type BReshmi VarmaNo ratings yet
- Nursing Students - Perception of The Stigma of Mental IllnessDocument7 pagesNursing Students - Perception of The Stigma of Mental IllnessMohammad Bashary M. GutocNo ratings yet
- Fredriksen Goldsen 2012 Disability Among Lesbian Gay and BiDocument6 pagesFredriksen Goldsen 2012 Disability Among Lesbian Gay and BiAsish DasNo ratings yet
- Relationships Between Beliefs About Medications and AdherenceDocument8 pagesRelationships Between Beliefs About Medications and Adherencenoor cahayaNo ratings yet
- Eating Disorders in Boys and MenFrom EverandEating Disorders in Boys and MenJason M. NagataNo ratings yet
- Mental Health Self-Care in Medical Students: A Comprehensive Look at Help-SeekingDocument17 pagesMental Health Self-Care in Medical Students: A Comprehensive Look at Help-SeekingNiLa AgustinaNo ratings yet
- Compet. de SaúdeDocument11 pagesCompet. de SaúdeLuciana OliveiraNo ratings yet
- Original Study: Gynecologic Issues of Adolescents With Down Syndrome, Autism, and Cerebral PalsyDocument5 pagesOriginal Study: Gynecologic Issues of Adolescents With Down Syndrome, Autism, and Cerebral PalsyZubaidah HassanNo ratings yet
- J Ctim 2020 102527Document8 pagesJ Ctim 2020 102527P17321203033 INGGRIT MAHENING DIRGANTARINo ratings yet
- Yahaya Mohammed Research 2024Document6 pagesYahaya Mohammed Research 2024emidibo4503No ratings yet
- Frailty 2: Management of Frailty: Opportunities, Challenges, and Future DirectionsDocument11 pagesFrailty 2: Management of Frailty: Opportunities, Challenges, and Future DirectionsGabriel MoraguesNo ratings yet
- Abstract: A Literature Search Shows Multiple Uses For Standardized Patients For Teaching and EvaluDocument5 pagesAbstract: A Literature Search Shows Multiple Uses For Standardized Patients For Teaching and EvaluwahyuraNo ratings yet
- Nihms 981224Document18 pagesNihms 981224miniypuntoNo ratings yet
- Preparing Tomorrow's Doctors To Care For Patients With Autism - 2016Document15 pagesPreparing Tomorrow's Doctors To Care For Patients With Autism - 2016Karel GuevaraNo ratings yet
- The General Practitioner and The Surgeon - Stereotypes and Medical SpecialtiesDocument10 pagesThe General Practitioner and The Surgeon - Stereotypes and Medical SpecialtiesCarol BusseNo ratings yet
- Abordagem Do Paciente Psiquiatrico Pelo ClínicoDocument24 pagesAbordagem Do Paciente Psiquiatrico Pelo ClínicoCintia AndradeNo ratings yet
- Compliance in Adolescents With Chronic Diseases: A ReviewDocument10 pagesCompliance in Adolescents With Chronic Diseases: A ReviewMaggy GarcíaNo ratings yet
- Medical Student Psychological Distress and Mental Illness Relative To The GeneralDocument11 pagesMedical Student Psychological Distress and Mental Illness Relative To The Generalmemmuse95No ratings yet
- Impact of Gender Bias On Male Nursing Students Competence of SkillsDocument13 pagesImpact of Gender Bias On Male Nursing Students Competence of Skillsapi-526815418No ratings yet
- A Two-Stage Epidemiological Study of Eating Disorders BAIRESDocument11 pagesA Two-Stage Epidemiological Study of Eating Disorders BAIRESGaby BarrozoNo ratings yet
- Effect - of - Health - Literacy - On - Decision-Making - Prefe HAMADDocument14 pagesEffect - of - Health - Literacy - On - Decision-Making - Prefe HAMADMOHD PERFECTNo ratings yet
- Decreasing PDFDocument10 pagesDecreasing PDFOscar Fernando Vargas HerreñoNo ratings yet
- Mond 2010klkoojljljlDocument20 pagesMond 2010klkoojljljlverghese17No ratings yet
- Erosion of Empathy in Medical SchoolDocument1 pageErosion of Empathy in Medical SchoolChristian ObandoNo ratings yet
- Position Statement Transgender Health PESDocument2 pagesPosition Statement Transgender Health PESxcarlosfxNo ratings yet
- Decision Making 5Document5 pagesDecision Making 5Yustina Ni Putu YusniawatiNo ratings yet
- Iacob, Folostina, Avram - 2022 - Caregiving PersonalityDocument11 pagesIacob, Folostina, Avram - 2022 - Caregiving PersonalityClauNo ratings yet
- Attitudes of Malaysian General Hospital Staff Towards Patients With Mental Illness and DiabetesDocument10 pagesAttitudes of Malaysian General Hospital Staff Towards Patients With Mental Illness and DiabetesragaNo ratings yet
- Nda Literature Review On Attitudes Towards DisabilityDocument6 pagesNda Literature Review On Attitudes Towards Disabilityc5sx83wsNo ratings yet
- Caring For Elderly Patients With Dementia Nursing PDFDocument11 pagesCaring For Elderly Patients With Dementia Nursing PDFAhmed MasoudNo ratings yet
- Caring For Elderly Patients With Dementia Nursing PDFDocument11 pagesCaring For Elderly Patients With Dementia Nursing PDFElla OrtizNo ratings yet
- Gender, Stress, Coping, and Health Behaviors: Measures DiscussionDocument1 pageGender, Stress, Coping, and Health Behaviors: Measures DiscussionHilda NuruzzamanNo ratings yet
- Periyakoil 2019Document28 pagesPeriyakoil 2019Da CuNo ratings yet
- Rebbe 2018Document8 pagesRebbe 2018Karen CárcamoNo ratings yet
- Getting Sexual and Gender Minority Health - Into The Brick and MorDocument262 pagesGetting Sexual and Gender Minority Health - Into The Brick and MorLieven VermeulenNo ratings yet
- Burden and Quality of Life of Caregivers For Hemodialysis PatientsDocument8 pagesBurden and Quality of Life of Caregivers For Hemodialysis PatientsAsim EisaNo ratings yet
- Evolution of Vulnerability: Implications for Sex Differences in Health and DevelopmentFrom EverandEvolution of Vulnerability: Implications for Sex Differences in Health and DevelopmentNo ratings yet
- Free Download: 7 Habits WorkbookDocument5 pagesFree Download: 7 Habits Workbookkuya sipit0% (2)
- 1010EZ FillableDocument5 pages1010EZ FillableFilozófus ÖnjelöltNo ratings yet
- Fall Prevention Program PDFDocument13 pagesFall Prevention Program PDFKusrini Kadar SyamsalamNo ratings yet
- Homeless Vet DirectoryDocument52 pagesHomeless Vet DirectoryEddie Goynes JrNo ratings yet
- Vha Fs Mission ActDocument3 pagesVha Fs Mission ActKBTXNo ratings yet
- House Hearing, 107TH Congress - H.R. 2716, Homeless Veterans Assistance Act of 2001 and H.R. 936, Heather French Henry Homeless Veterans Assistance ActDocument270 pagesHouse Hearing, 107TH Congress - H.R. 2716, Homeless Veterans Assistance Act of 2001 and H.R. 936, Heather French Henry Homeless Veterans Assistance ActScribd Government DocsNo ratings yet
- Testing For Primary Hyperaldosteronism and MRA TX Annals 2020Document10 pagesTesting For Primary Hyperaldosteronism and MRA TX Annals 2020Miri PravdaNo ratings yet
- VHA Directive 1083 Notification of Med Malpractice Tort Claims To Involved Pract 6 14 17 1Document13 pagesVHA Directive 1083 Notification of Med Malpractice Tort Claims To Involved Pract 6 14 17 1Arvin TerrellNo ratings yet
- Va259 14 R 0224 002Document53 pagesVa259 14 R 0224 002raulneti1984No ratings yet
- Knowledge, Attitudes, and Practices of Bedside Nursing Staff PDFDocument4 pagesKnowledge, Attitudes, and Practices of Bedside Nursing Staff PDFwindysandy100% (1)
- Guideline For Rehabilitation Lower Limb AmputeesDocument166 pagesGuideline For Rehabilitation Lower Limb Amputeesmihaela_moldova9128100% (1)
- Goal Setting Referral AssignmentDocument4 pagesGoal Setting Referral Assignmentapi-309598310No ratings yet
- Women at WarDocument393 pagesWomen at WarJorge HerrejónNo ratings yet
- Ethical Leadership Fostering An Ethical Environment and Culture 20070808Document60 pagesEthical Leadership Fostering An Ethical Environment and Culture 20070808Maureen O'BrienNo ratings yet
- Bryant Seamon, PT, DPT, NCS, CSCS: EducationDocument6 pagesBryant Seamon, PT, DPT, NCS, CSCS: Educationapi-324333142No ratings yet
- Tester's State of Veterans in Montana ReportDocument26 pagesTester's State of Veterans in Montana ReportsenatortesterNo ratings yet
- US - National Action Plan For Adverse Drug Event PreventionDocument190 pagesUS - National Action Plan For Adverse Drug Event PreventionClaudia NogueiraNo ratings yet
- VA Form 10-7959cDocument2 pagesVA Form 10-7959cbaluchiifNo ratings yet
- Hepatitis C Education Class - 2009Document64 pagesHepatitis C Education Class - 2009BENNo ratings yet
- Veterans Affairs Outpatient Scheduling PolicyDocument11 pagesVeterans Affairs Outpatient Scheduling PolicyMail TribuneNo ratings yet
- Mental Health Facilities Design GuideDocument317 pagesMental Health Facilities Design GuideIDrHotdog100% (1)
- Vba 21P 534ez AreDocument14 pagesVba 21P 534ez AreARNOLD GONZALESNo ratings yet
- GEM Model of CareDocument58 pagesGEM Model of CareKhoirun NisyakNo ratings yet
- 2015 Women of Distinction Contemporary BookDocument84 pages2015 Women of Distinction Contemporary BookNew York SenateNo ratings yet
- Interior Design ManualDocument96 pagesInterior Design ManualLaisattrooklai Phisit94% (17)
- Using Business Intelligence: The Strategic Use of Analytics in GovernmentDocument6 pagesUsing Business Intelligence: The Strategic Use of Analytics in GovernmentIBMGovernmentNo ratings yet
- DBQ Fact SheetDocument1 pageDBQ Fact SheetEd BallNo ratings yet
- CMAPP Analysis Good OneDocument5 pagesCMAPP Analysis Good OneM annonymousNo ratings yet
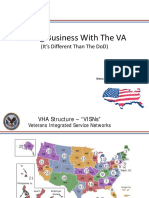
- Keynote Steve Elliott, Doing Business With The VA (It's Different Than The DoD), VA SAME Brief FinalDocument22 pagesKeynote Steve Elliott, Doing Business With The VA (It's Different Than The DoD), VA SAME Brief FinalSAMETampaBayNo ratings yet
- Caregiver Workbook V3 Module 5Document14 pagesCaregiver Workbook V3 Module 5Pablo RodriguezNo ratings yet