You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Kids Box New Generation 3 Pupils BookDocument97 pagesKids Box New Generation 3 Pupils BookMicaela Corado Dedo100% (5)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Power of Attention PDFDocument158 pagesPower of Attention PDFSteven Droullard100% (9)
- FAST-Alzheimer - S Disease Staging Tool PDFDocument2 pagesFAST-Alzheimer - S Disease Staging Tool PDFArumDesiPratiwiNo ratings yet
- Living From Truth A Manual For Masters of Long Enlightenment IntensivesDocument116 pagesLiving From Truth A Manual For Masters of Long Enlightenment IntensivesZeljko Zex Malinovic100% (1)
- WC BPR - Prevention and Management of Diabetic Foot Ulcers 1573r4e FinalDocument68 pagesWC BPR - Prevention and Management of Diabetic Foot Ulcers 1573r4e FinalArumDesiPratiwiNo ratings yet
- Editorial: Clinical Neurophysiology in Alzheimer's DiseaseDocument2 pagesEditorial: Clinical Neurophysiology in Alzheimer's DiseaseArumDesiPratiwiNo ratings yet
- 9149StatlerMentalStatus PDFDocument5 pages9149StatlerMentalStatus PDFArumDesiPratiwiNo ratings yet
- Lembar Penilaian Praktik Profesi Medikal Jurusan Keperawatan Fkub Ta 2014/2015Document1 pageLembar Penilaian Praktik Profesi Medikal Jurusan Keperawatan Fkub Ta 2014/2015ArumDesiPratiwiNo ratings yet
- Solunum 15 1 1 4Document4 pagesSolunum 15 1 1 4ArumDesiPratiwiNo ratings yet
- Mini Mental State EvaluationDocument1 pageMini Mental State EvaluationArumDesiPratiwiNo ratings yet
- Postnatal Care (Puerperium) : Common Puerperal ProblemsDocument4 pagesPostnatal Care (Puerperium) : Common Puerperal ProblemsArumDesiPratiwiNo ratings yet
- Social Sciences-Grade 9 Geography Worksheet May 2020Document7 pagesSocial Sciences-Grade 9 Geography Worksheet May 2020agangdayimaniNo ratings yet
- SensorsDocument69 pagesSensorsRiahi Rezeg100% (1)
- Santrock Report SCRATCHDocument23 pagesSantrock Report SCRATCHAngela YaraNo ratings yet
- Compiler LabDocument63 pagesCompiler LabAbhishek YadavNo ratings yet
- Fairview Terminal PhaseII Expansion Project Report - Oct2012Document436 pagesFairview Terminal PhaseII Expansion Project Report - Oct2012NewsroomNo ratings yet
- Aqa 83622 SMS PDFDocument14 pagesAqa 83622 SMS PDFT SolomonNo ratings yet
- Fortified TeaDocument12 pagesFortified TeaRahul TripathiNo ratings yet
- Tonepad Pedal RATDocument0 pagesTonepad Pedal RATJose David DíazNo ratings yet
- Review of Status of Advanced Materials (Cost)Document60 pagesReview of Status of Advanced Materials (Cost)enriquesantaolallaNo ratings yet
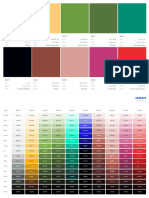
- Color 1 Color 2 Color 3 Color 4 Color 5: RGB Cmyk Name RGB Cmyk Name RGB Cmyk Name RGB Cmyk Name RGB Cmyk NameDocument4 pagesColor 1 Color 2 Color 3 Color 4 Color 5: RGB Cmyk Name RGB Cmyk Name RGB Cmyk Name RGB Cmyk Name RGB Cmyk NameValentina TorresNo ratings yet
- Concrete Formwork SystemsDocument252 pagesConcrete Formwork SystemsAsraf KacakNo ratings yet
- HVDC Ground ElectrodeDocument13 pagesHVDC Ground ElectrodeHeather CarterNo ratings yet
- Unit 2Document7 pagesUnit 2Hind HindouNo ratings yet
- Qualcast Trucks Catalog2015Document188 pagesQualcast Trucks Catalog2015Edwin Javier Garavito100% (2)
- How To Apply Transit Validation StandardsDocument6 pagesHow To Apply Transit Validation StandardsBechir OuhibiNo ratings yet
- Yaya Maimouna RizalDocument5 pagesYaya Maimouna RizalKriselle Ann CalsoNo ratings yet
- Literature Review Benefits Outdoor PlayDocument7 pagesLiterature Review Benefits Outdoor Playfvg6kcwy100% (1)
- Coral Reef Restoration A Guide To EffectDocument56 pagesCoral Reef Restoration A Guide To EffectDavid Higuita RamirezNo ratings yet
- Yle Movers PostersDocument2 pagesYle Movers PostersVictoria100% (2)
- Overview of The DSM 5Document68 pagesOverview of The DSM 5khalpopoNo ratings yet
- PM Fellowship Call For ProposalDocument36 pagesPM Fellowship Call For ProposalShivashankar HiremathNo ratings yet
- ATV61 Communication Parameters en V5.8 IE29Document126 pagesATV61 Communication Parameters en V5.8 IE29Anonymous kiyxz6eNo ratings yet
- Ncert Summary Class 12th PhysicsDocument29 pagesNcert Summary Class 12th Physicsmeghraj.socialNo ratings yet
- Gsic Lexus Is350300 250 200d Gse 202122 Ale20 2010 2012Document22 pagesGsic Lexus Is350300 250 200d Gse 202122 Ale20 2010 2012joelsimpson171001toy100% (137)
- 500kVA Dyn5Document1 page500kVA Dyn5edwardNo ratings yet
- The Times ProjectionDocument5 pagesThe Times ProjectionBelinda NiuNo ratings yet
- Nature and Scope of Analytical ChemistryDocument4 pagesNature and Scope of Analytical Chemistryjay c100% (1)