You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Surgical Emergencies in Clinical Practice (2013) 2Document225 pagesSurgical Emergencies in Clinical Practice (2013) 2noir100% (2)
- Usmle CCSDocument224 pagesUsmle CCSShane Allen100% (5)
- Pancreatitis: (Alterations in Metabolic and Endocrine Functions)Document7 pagesPancreatitis: (Alterations in Metabolic and Endocrine Functions)Jorie Roco0% (1)
- Pancreatic PathologyDocument7 pagesPancreatic Pathologyzeroun24100% (1)
- NCPDocument11 pagesNCPJaziel Remo100% (1)
- General Surgery MCQ SaudiDocument57 pagesGeneral Surgery MCQ SaudiAsif Newaz100% (6)
- Acute PancreatitisDocument78 pagesAcute Pancreatitisagus100% (1)
- Care of Adults 27 Gastrointestinal ManagementDocument33 pagesCare of Adults 27 Gastrointestinal ManagementGaras AnnaBerniceNo ratings yet
- Careplan Acute PancreatitisDocument2 pagesCareplan Acute PancreatitisBSN 2014100% (4)
- Henry's Clinical Diagnosis and Management by Laboratory Methods Twenty-Third Edition 2017Document20 pagesHenry's Clinical Diagnosis and Management by Laboratory Methods Twenty-Third Edition 2017Denise GuevaraNo ratings yet
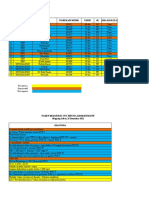
- Mapping Minggu, 26 Desember 2021Document3 pagesMapping Minggu, 26 Desember 2021Suis MionooNo ratings yet
- Mapping Jum'at, 24 Desember 2021Document4 pagesMapping Jum'at, 24 Desember 2021Suis MionooNo ratings yet
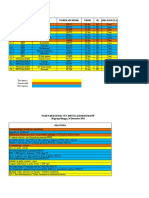
- Mapping Sabtu, 25 Desember 2021Document3 pagesMapping Sabtu, 25 Desember 2021Suis MionooNo ratings yet
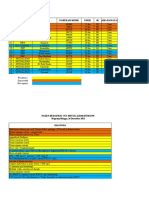
- Mapping Senin, 27 Desember 2021Document3 pagesMapping Senin, 27 Desember 2021Suis MionooNo ratings yet
- An Anth 2016Document32 pagesAn Anth 2016Suis MionooNo ratings yet
- Pone 0233641Document15 pagesPone 0233641Suis MionooNo ratings yet
- Abruptio Placenta Retrospective Study: Maternal and Fetal OutcomeDocument4 pagesAbruptio Placenta Retrospective Study: Maternal and Fetal OutcomeSuis MionooNo ratings yet
- fef9d16481553837049874e411a5556eDocument17 pagesfef9d16481553837049874e411a5556eSuis MionooNo ratings yet
- Case ReportDocument9 pagesCase ReportSuis MionooNo ratings yet
- Pos Ok Hova 2012Document1 pagePos Ok Hova 2012Suis MionooNo ratings yet
- Hill 2020Document2 pagesHill 2020Suis MionooNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument7 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologySuis MionooNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument5 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologySuis MionooNo ratings yet
- Nutrients: of Mice and Men-The Physiology, Psychology, and Pathology of OverhydrationDocument14 pagesNutrients: of Mice and Men-The Physiology, Psychology, and Pathology of OverhydrationSuis MionooNo ratings yet
- MCN 13157Document8 pagesMCN 13157Suis MionooNo ratings yet
- Research Open Access: Samoni Et Al. Critical Care (2016) 20:95 DOI 10.1186/s13054-016-1269-6Document8 pagesResearch Open Access: Samoni Et Al. Critical Care (2016) 20:95 DOI 10.1186/s13054-016-1269-6Suis MionooNo ratings yet
- Diagnostics: Pyonephrosis Ultrasound and Computed Tomography Features: A Pictorial ReviewDocument12 pagesDiagnostics: Pyonephrosis Ultrasound and Computed Tomography Features: A Pictorial ReviewSuis MionooNo ratings yet
- The Acinar-Ductal Tango in The Pathogenesis of Acute PancreatitisDocument10 pagesThe Acinar-Ductal Tango in The Pathogenesis of Acute Pancreatitispruebaprueba321765No ratings yet
- Acute Pancreatitis. Lancet Seminar Sept 5, 2020Document9 pagesAcute Pancreatitis. Lancet Seminar Sept 5, 2020Luis Henrique SalesNo ratings yet
- PancreatiteTRADUZIR - ESPEN Guideline On Clinical Nutrition in Acute and Chronic PancreatitisDocument20 pagesPancreatiteTRADUZIR - ESPEN Guideline On Clinical Nutrition in Acute and Chronic Pancreatitisthaisagoraer1No ratings yet
- Pancreatita AcutaDocument17 pagesPancreatita AcutaAdina TomaNo ratings yet
- PANCREATITISDocument38 pagesPANCREATITISVEDHIKAVIJAYANNo ratings yet
- Data StreamDocument87 pagesData StreamL-Va AndesNo ratings yet
- Diseases of The Biliary Tract: Hepatic, Biliary Tract, and Pancreatic Dysfunction: Nursing ManagementDocument57 pagesDiseases of The Biliary Tract: Hepatic, Biliary Tract, and Pancreatic Dysfunction: Nursing ManagementMichael Baylon DueñasNo ratings yet
- Acute PancreatitisDocument25 pagesAcute PancreatitisSunil YadavNo ratings yet
- Comparison of The Major CarbapenemsDocument28 pagesComparison of The Major CarbapenemsAnjum MushtaqNo ratings yet
- Daniel Da Costa Gidi: Extracción Endoscópica de Cálculos Pancreáticos en Pancreatitis Crónica para Evitar ReagudizacionesDocument5 pagesDaniel Da Costa Gidi: Extracción Endoscópica de Cálculos Pancreáticos en Pancreatitis Crónica para Evitar ReagudizacionesDr Daniel da costa Gidi opinionesNo ratings yet
- Nutritional Managements of Gastrointestinal Diseases/DisordersDocument54 pagesNutritional Managements of Gastrointestinal Diseases/Disordersendang sry09No ratings yet
- Fluid Resuscitation in Acoute Pancreatitis - PrefinalDocument35 pagesFluid Resuscitation in Acoute Pancreatitis - PrefinalSahir BNo ratings yet
- DR Is-Acute PancreatitisDocument11 pagesDR Is-Acute PancreatitisSemestaNo ratings yet
- Acute Pancreatitis (Acute Pancreatic Necrosis)Document12 pagesAcute Pancreatitis (Acute Pancreatic Necrosis)sosotarab2No ratings yet
- UntitledDocument2 pagesUntitledAelysa PabloNo ratings yet
- Acute Pancreatitis (Acute Pancreatic Necrosis)Document12 pagesAcute Pancreatitis (Acute Pancreatic Necrosis)Amol DhopteNo ratings yet
- Acute PancreatitisDocument46 pagesAcute PancreatitisNurul Azizah MNo ratings yet
- Scoring PancreatitisDocument3 pagesScoring PancreatitisAgung HNo ratings yet
- MCQ Block 13Document15 pagesMCQ Block 13Liliana Surya Fatimah0% (1)
- Askep PankreatitisDocument48 pagesAskep PankreatitisYeni DwiNo ratings yet