You might also like
- McWilliams (2009)Document4 pagesMcWilliams (2009)Stacy Lanier100% (1)
- Peer ReviewDocument24 pagesPeer ReviewSimon Dzokoto100% (1)
- Disease Prevention and Control: Dr.K.Arulanandem Lecturer/CoordinatorDocument30 pagesDisease Prevention and Control: Dr.K.Arulanandem Lecturer/Coordinatorv_vijayakanth7656No ratings yet
- SITHKOP005 - Coordinate CookingDocument78 pagesSITHKOP005 - Coordinate Cookingsheyla0% (1)
- Conversation Between Doctor and PatientDocument5 pagesConversation Between Doctor and PatientTeeeeHeeee100% (1)
- Association Between Perioperative Fluid Management and Patient Outcomes: A Multicentre Retrospective StudyDocument10 pagesAssociation Between Perioperative Fluid Management and Patient Outcomes: A Multicentre Retrospective Studyana mariaNo ratings yet
- Effects of Fluid Balance On Prognosis of Acute Respiratory Distress Syndrome Patients Secondary To SepsisDocument7 pagesEffects of Fluid Balance On Prognosis of Acute Respiratory Distress Syndrome Patients Secondary To SepsisPIR BanjarmasinNo ratings yet
- 2018 Article 2099Document10 pages2018 Article 2099igariok06No ratings yet
- ContentServer 002Document17 pagesContentServer 002RosihayatiNo ratings yet
- Acumulacion de Liquidos Como Evento Adverso Renal en SepsisDocument12 pagesAcumulacion de Liquidos Como Evento Adverso Renal en SepsisJaime RomeroNo ratings yet
- Ibi JurnalDocument9 pagesIbi JurnalRiski Pradika 2017No ratings yet
- Effect of Combined Renin Angiotensin Aldosterone Inhibitors and Diuretic Treatment Among Patients Hospitalized With Sars-Cov-2 Infection Covid-19Document16 pagesEffect of Combined Renin Angiotensin Aldosterone Inhibitors and Diuretic Treatment Among Patients Hospitalized With Sars-Cov-2 Infection Covid-19Muhammad Halil GibranNo ratings yet
- 2019 Article 1596Document9 pages2019 Article 1596Arina FitrianiNo ratings yet
- A Longitudinal Change of Syndecan-1 Predicts Risk of Acute Respiratory Distress Syndrome and Cumulative Fluid Balance in Patients With Septic Shock - A Preliminary StudyDocument9 pagesA Longitudinal Change of Syndecan-1 Predicts Risk of Acute Respiratory Distress Syndrome and Cumulative Fluid Balance in Patients With Septic Shock - A Preliminary StudyPIR BanjarmasinNo ratings yet
- Congestión Por LíquidosDocument10 pagesCongestión Por Líquidosandres ruizNo ratings yet
- Diagnosis FluidDocument14 pagesDiagnosis FluidCristianMP96No ratings yet
- Continuous Renal Replacement Therapy Among Patients With COVID-19 and Acute Kidney InjuryDocument8 pagesContinuous Renal Replacement Therapy Among Patients With COVID-19 and Acute Kidney InjuryPIR BanjarmasinNo ratings yet
- Central Venous Pressure and Acute Kidney Injury in Critically Ill Patients With Multiple Comorbidities A Large Retrospective Cohort StudyDocument10 pagesCentral Venous Pressure and Acute Kidney Injury in Critically Ill Patients With Multiple Comorbidities A Large Retrospective Cohort Studyady suciptoNo ratings yet
- Ficha Bibliografica UciDocument8 pagesFicha Bibliografica Ucimaria castillo lizcanoNo ratings yet
- Fluid Management in Critically Ill Patients: The Role of Extravascular Lung Water, Abdominal Hypertension, Capillary Leak, and Fluid BalanceDocument12 pagesFluid Management in Critically Ill Patients: The Role of Extravascular Lung Water, Abdominal Hypertension, Capillary Leak, and Fluid BalanceShamini ShanmugalingamNo ratings yet
- Gastroenterology: World Journal ofDocument14 pagesGastroenterology: World Journal ofrahul krishnanNo ratings yet
- International Journal of Cardiology: SciencedirectDocument6 pagesInternational Journal of Cardiology: SciencedirectRobsonBorgesNo ratings yet
- Relationship Between PlateletLymphocyte Ratio andDocument5 pagesRelationship Between PlateletLymphocyte Ratio andFranz TariganNo ratings yet
- Association Between Fluid Overload and SOFA Score Kinetics in Septic Shock Patients: A Retrospective Multicenter StudyDocument18 pagesAssociation Between Fluid Overload and SOFA Score Kinetics in Septic Shock Patients: A Retrospective Multicenter StudydaliaNo ratings yet
- AKI Urinary Biomarkers in COVID 19 2020 PreliminaryDocument4 pagesAKI Urinary Biomarkers in COVID 19 2020 PreliminaryMg GfNo ratings yet
- Epidemio AkiDocument10 pagesEpidemio AkiSoniamartilovaNo ratings yet
- Research Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology FindingsDocument9 pagesResearch Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology Findings28121998No ratings yet
- Journal of Critical Care: Biao Wang, MD, Gang Chen, MD, Yifei Cao, MD, Jiping Xue, MD, Jia Li, MD, Yunfu Wu, MDDocument5 pagesJournal of Critical Care: Biao Wang, MD, Gang Chen, MD, Yifei Cao, MD, Jiping Xue, MD, Jia Li, MD, Yunfu Wu, MDpramastutiNo ratings yet
- Journal Pone 0243782Document12 pagesJournal Pone 0243782wenyNo ratings yet
- Extent, Risk Factors, and Outcome of Fluid Overload After Pediatric Heart SurgeryDocument9 pagesExtent, Risk Factors, and Outcome of Fluid Overload After Pediatric Heart SurgeryAngelica Lucero OrtizNo ratings yet
- Abdominal Sepsis Prognostic FactorDocument6 pagesAbdominal Sepsis Prognostic FactorPrasojo JojoNo ratings yet
- CCM 0000000000001948Document8 pagesCCM 0000000000001948KarenMartinezNo ratings yet
- Systemic Immune-In Ammatory Index Predicts Prognosis of Patients With COVID-19: A Retrospective StudyDocument37 pagesSystemic Immune-In Ammatory Index Predicts Prognosis of Patients With COVID-19: A Retrospective StudyJuliana SanjayaNo ratings yet
- Increased Fluid Administration in The First TH Ree Hours of Sepsis Resuscitation Is Associated With Reduced MortalityDocument8 pagesIncreased Fluid Administration in The First TH Ree Hours of Sepsis Resuscitation Is Associated With Reduced MortalityAzmachamberAzmacareNo ratings yet
- Electrocardiometry For Hemodynamic Categorization and Assessment of Fluid Responsiveness in Pediatric Septic Shock - A Pilot Observational StudyDocument8 pagesElectrocardiometry For Hemodynamic Categorization and Assessment of Fluid Responsiveness in Pediatric Septic Shock - A Pilot Observational StudyMarselya GaniNo ratings yet
- Saving Critically Ill COVID-19 Patients With Mechanical Circulatory SupportDocument11 pagesSaving Critically Ill COVID-19 Patients With Mechanical Circulatory SupportSara MendesNo ratings yet
- Impact of Early Mean Arterial Pressure Level On Severe Acute Kidney Injury Occurrence After Out-Of-Hospital Cardiac ArrestDocument10 pagesImpact of Early Mean Arterial Pressure Level On Severe Acute Kidney Injury Occurrence After Out-Of-Hospital Cardiac ArrestElizabeth PedruezaNo ratings yet
- Original ContributionDocument6 pagesOriginal ContributionClaudia IsabelNo ratings yet
- Apa GituDocument8 pagesApa GituRiadi RifqiNo ratings yet
- 10.1007@s11739 019 02196 ZDocument10 pages10.1007@s11739 019 02196 ZMaharani Sari NastitiNo ratings yet
- WJCCM 10 22Document14 pagesWJCCM 10 22Syawaluddin sakti maulanaNo ratings yet
- CC 9070Document15 pagesCC 9070ossinNo ratings yet
- 2014 Article 639Document8 pages2014 Article 639Anida HasnaNo ratings yet
- Positive Effect of Care Bundles On Patients With Central Venous Catheter Insertions at A Tertiary Hospital in Beijing, ChinaDocument10 pagesPositive Effect of Care Bundles On Patients With Central Venous Catheter Insertions at A Tertiary Hospital in Beijing, ChinaElfina NataliaNo ratings yet
- Infectious DiseasesDocument9 pagesInfectious DiseasesMaharani Sari NastitiNo ratings yet
- Haemodialysis With On-Line Monitoring EquipmentDocument12 pagesHaemodialysis With On-Line Monitoring EquipmentConnie Alva GutierrezNo ratings yet
- Messina Et Al-2022-Intensive Care Medicine ExperimentalDocument15 pagesMessina Et Al-2022-Intensive Care Medicine ExperimentalAna Belén Viteri luzuriagaNo ratings yet
- The Association Between Intravenous Fluid Resuscitation and Mortality in Older Emergency Department Patients With Suspected InfectionDocument8 pagesThe Association Between Intravenous Fluid Resuscitation and Mortality in Older Emergency Department Patients With Suspected InfectiongabbynengNo ratings yet
- 10 1111@ijlh 13273 PDFDocument7 pages10 1111@ijlh 13273 PDFMoonika TodinganNo ratings yet
- In Critically Ill Adult Patients Community-Acquired Bloodstream InfectionDocument12 pagesIn Critically Ill Adult Patients Community-Acquired Bloodstream InfectionNeliel NoraNo ratings yet
- 1 RifDocument29 pages1 RifRifdah AmalinaNo ratings yet
- Red Cell Distribution in Critically Ill Patients With Chronic Obstructive Pulmonary DiseaseDocument9 pagesRed Cell Distribution in Critically Ill Patients With Chronic Obstructive Pulmonary Diseaserbatjun576No ratings yet
- Diagnosis of Fluid Overload: From Conventional To Contemporary ConceptsDocument14 pagesDiagnosis of Fluid Overload: From Conventional To Contemporary Conceptsbenitez1228No ratings yet
- The Prognostic Value of The SOFA Score in PatientsDocument24 pagesThe Prognostic Value of The SOFA Score in PatientsYuri SadewoNo ratings yet
- Clinical Efficacy of Intravenous Immunoglobulin Therapy in Critical Patients With COVID-19: A Multicenter Retrospective Cohort StudyDocument25 pagesClinical Efficacy of Intravenous Immunoglobulin Therapy in Critical Patients With COVID-19: A Multicenter Retrospective Cohort StudyRudy Cagua GuerreroNo ratings yet
- Journal Pone 0035634Document5 pagesJournal Pone 0035634Nathaly AráuzNo ratings yet
- Hydrocortisone, Vitamin C, and Thiamine For The Treatment of Severe Sepsis and Septic ShockDocument10 pagesHydrocortisone, Vitamin C, and Thiamine For The Treatment of Severe Sepsis and Septic Shockmmmaw mmNo ratings yet
- Acute Kidney Injury Due To Diarrheal Illness Requiring Hospitalization: Data From The National Inpatient SampleDocument8 pagesAcute Kidney Injury Due To Diarrheal Illness Requiring Hospitalization: Data From The National Inpatient SampleCherry SmileNo ratings yet
- Fluid Resuscitation With Balanced Crystalloids Versus Normal Saline in Critically Ill Patients: A Systematic Review and Meta-AnalysisDocument10 pagesFluid Resuscitation With Balanced Crystalloids Versus Normal Saline in Critically Ill Patients: A Systematic Review and Meta-AnalysisSyamil ImtiyaziNo ratings yet
- Initial Hemodynamic Profiles of Children with Dengue Shock SyndromeDocument7 pagesInitial Hemodynamic Profiles of Children with Dengue Shock SyndromeEly macNo ratings yet
- Fluid Management in ARDS: An Evaluation of Current Practice and The Association Between Early Diuretic Use and Hospital MortalityDocument11 pagesFluid Management in ARDS: An Evaluation of Current Practice and The Association Between Early Diuretic Use and Hospital MortalitywasiNo ratings yet
- Lung Protective Mechanical Ventilation StrategiesDocument4 pagesLung Protective Mechanical Ventilation StrategiesAnne Julia AgustinNo ratings yet
- HDFVVC EfectoDocument11 pagesHDFVVC Efectogiseladelarosa2006No ratings yet
- Sup ...Document4 pagesSup ...Faisyal RezaNo ratings yet
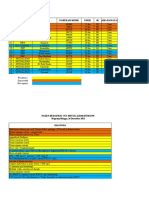
- Mapping Senin, 27 Desember 2021Document3 pagesMapping Senin, 27 Desember 2021Suis MionooNo ratings yet
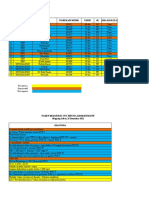
- Mapping Sabtu, 25 Desember 2021Document3 pagesMapping Sabtu, 25 Desember 2021Suis MionooNo ratings yet
- ANC Guideline PresentationDocument46 pagesANC Guideline Presentationjessica_siahaan_1No ratings yet
- PATIENT LISTINGDocument3 pagesPATIENT LISTINGSuis MionooNo ratings yet
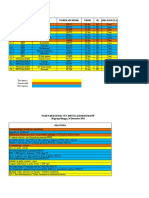
- Mapping Jum'at, 24 Desember 2021Document4 pagesMapping Jum'at, 24 Desember 2021Suis MionooNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument8 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologySuis MionooNo ratings yet
- Pos Ok Hova 2012Document1 pagePos Ok Hova 2012Suis MionooNo ratings yet
- Case ReportDocument9 pagesCase ReportSuis MionooNo ratings yet
- Brain Surgery: Here Is Where Your Presentation BeginsDocument54 pagesBrain Surgery: Here Is Where Your Presentation BeginsJabelle Mae DoteNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument5 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologySuis MionooNo ratings yet
- Pone 0233641Document15 pagesPone 0233641Suis MionooNo ratings yet
- An Anth 2016Document32 pagesAn Anth 2016Suis MionooNo ratings yet
- AHAASA CVDNH Guidelines 2019 PDFDocument75 pagesAHAASA CVDNH Guidelines 2019 PDFJessica WiryantoNo ratings yet
- Abruptio Placenta Retrospective Study: Maternal and Fetal OutcomeDocument4 pagesAbruptio Placenta Retrospective Study: Maternal and Fetal OutcomeSuis MionooNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument7 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologySuis MionooNo ratings yet
- Biomarkers predict cervical length and bacteriaDocument2 pagesBiomarkers predict cervical length and bacteriaSuis MionooNo ratings yet
- fef9d16481553837049874e411a5556eDocument17 pagesfef9d16481553837049874e411a5556eSuis MionooNo ratings yet
- Modul 10 - Pengelolaan NyeriDocument96 pagesModul 10 - Pengelolaan NyeriAyu PermataNo ratings yet
- Preeclampsia 2 PDFDocument6 pagesPreeclampsia 2 PDFaxel jovito siburianNo ratings yet
- Sin TítuloDocument8 pagesSin TítuloZeptalanNo ratings yet
- Risk Factors and Maternal-Fetal Outcomes of Placental AbruptionDocument5 pagesRisk Factors and Maternal-Fetal Outcomes of Placental AbruptionSuis MionooNo ratings yet
- Professional Scrapbook Meeting by SlidesgoDocument47 pagesProfessional Scrapbook Meeting by SlidesgoRyduan Cristophers Sara GutierrezNo ratings yet
- MCN 13157Document8 pagesMCN 13157Suis MionooNo ratings yet
- Modul 10 - Pengelolaan NyeriDocument96 pagesModul 10 - Pengelolaan NyeriAyu PermataNo ratings yet
- Nutrients: of Mice and Men-The Physiology, Psychology, and Pathology of OverhydrationDocument14 pagesNutrients: of Mice and Men-The Physiology, Psychology, and Pathology of OverhydrationSuis MionooNo ratings yet
- 8266 42109 7 PBDocument11 pages8266 42109 7 PBSuis MionooNo ratings yet
- TRR 6655 TrfsDocument2 pagesTRR 6655 TrfsSuis MionooNo ratings yet
- Fluid Composition and Clinical Effects PDFDocument15 pagesFluid Composition and Clinical Effects PDFMace HernandezNo ratings yet
- Radiology of Acute Pancreatitis TodayDocument10 pagesRadiology of Acute Pancreatitis TodaySuis MionooNo ratings yet
- Hipertensi KebidananDocument77 pagesHipertensi KebidananNINING ALKOMAHNo ratings yet
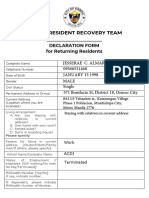
- RRT Declaration Form UpdatedDocument2 pagesRRT Declaration Form UpdatedShayne Jessemae AlmarioNo ratings yet
- FCE TestDocument10 pagesFCE TestNguyen TrangNo ratings yet
- Barret's Syndrome Case ReportDocument3 pagesBarret's Syndrome Case ReportResearch ParkNo ratings yet
- Padlan Getigan and PartnersDocument4 pagesPadlan Getigan and PartnersMichaelandKaye DanaoNo ratings yet
- Lesson 52ND Q ManifestoDocument30 pagesLesson 52ND Q ManifestoLiya Mae SantiagoNo ratings yet
- Emocional Health: Emotiona L Health Activities at HomeDocument1 pageEmocional Health: Emotiona L Health Activities at HomeMarianne Herzfeld FajardoNo ratings yet
- UKFP 2024 Applicant HandbookDocument20 pagesUKFP 2024 Applicant HandbookS Abi GunnamNo ratings yet
- Ncp. Pedia.Document2 pagesNcp. Pedia.Czarina MayoNo ratings yet
- Teks EksposisiDocument2 pagesTeks EksposisiHadiq IbnuNo ratings yet
- Hyperbilirubinemia (Gerardo, Maria Maricar P)Document11 pagesHyperbilirubinemia (Gerardo, Maria Maricar P)Carlojay IniegoNo ratings yet
- Doh ProgramsDocument45 pagesDoh ProgramsVon Andre AposagaNo ratings yet
- MSCDFSM Prog. GuideDocument108 pagesMSCDFSM Prog. Guidesamraju1No ratings yet
- NCP KateDor NewDocument6 pagesNCP KateDor NewSteffi GolezNo ratings yet
- Gordon'S Functional Health PatternDocument10 pagesGordon'S Functional Health PatternDave SapladNo ratings yet
- Using Technology To Study Cellular and Molecular BiologyDocument138 pagesUsing Technology To Study Cellular and Molecular BiologybheeshmatNo ratings yet
- Enc 1102 ReasearchdfinalDocument9 pagesEnc 1102 Reasearchdfinalapi-507725488No ratings yet
- Giving Advice 2Document11 pagesGiving Advice 2Devi CintyaNo ratings yet
- Graphic Organizer ExampleDocument1 pageGraphic Organizer Exampleapi-398530613No ratings yet
- 1.6 - Maslow's Hierarchy of NeedsDocument3 pages1.6 - Maslow's Hierarchy of NeedsOkoye CynthiaNo ratings yet
- Understanding Acute Leukemia: Signs, Symptoms and TreatmentDocument46 pagesUnderstanding Acute Leukemia: Signs, Symptoms and TreatmentMaica LectanaNo ratings yet
- Orthopaedics Subspecialties 2Document3 pagesOrthopaedics Subspecialties 2Neung ThadaNo ratings yet
- Woodend Nursery Day Care of ChildrenDocument11 pagesWoodend Nursery Day Care of ChildrenSRARNo ratings yet
- Sister Callista RoyDocument17 pagesSister Callista RoyAbhee CalimagNo ratings yet
- Fitness Goals and Target Heart RateDocument8 pagesFitness Goals and Target Heart RateRuben Rosendal De AsisNo ratings yet